Article Text

Statistics from Altmetric.com
Introduction
In children it is often essential to recognise serious infections at an early stage to reduce possible life-threatening complications.
C reactive protein (CRP) is an acute-phase protein, secreted in response to any infection or inflammation.1 Venous blood sampling can be difficult in children in ambulatory care. A point-of-care (POC) test, provided at the bedside, presents an immediate result from a droplet of blood and is especially useful in children.
Previous generations of POC CRP tests have shown good correlation with standard laboratory tests in studies in primary care and emergency departments.1–3 Measuring CRP could contribute to clinical decision-making in diagnosing serious infection.4
We determined the analytical accuracy (closeness of the agreement between the measurement results and a true value) and user-friendliness of the Afinion CRP test (on the Afinion AS100 Analyzer, Alere, USA), in children and adults.
Methods
To assess analytical accuracy, we performed POC CRP tests in children (aged 1 month–18 years) admitted to an inpatient paediatric unit or attending an outpatient paediatric clinic, and in adults (aged 18–65 years) attending a general practice surgery. User-friendliness was evaluated by the participating general practitioners.
This study was approved by the ethical review board of the KU Leuven, under reference ML8239.
Afinion CRP test
The Afinion CRP Test Cartridge consists of a 1.5 µL glass capillary and a reagent container. The result is available within 4 min and the measuring range for CRP is 5–200 mg/L. One physician (JYV) performed all POC CRP tests in children, executing every finger stick in a similar fashion (lateral side of the index finger with a small 28 Gauge spring loaded needle). For internal quality control, a positive sample was measured regularly to confirm the efficacy and correct performance of the test.
The accuracy was assessed comparing the results of the Afinion CRP test and the venous sample immunoturbidimetric CRP test with antibody-carrying latex particles tested performed on a Cobas c702 (Roche Diagnostics, Switzerland). The correlation was analysed and plotted using the Passing–Bablok linear regression method and the differences and agreement according to the Bland–Altman method.
In three general practice surgeries, 10 physicians performed POC CRP tests. They were asked to fill out a questionnaire, consisting of a 5-point Likert scale, based on device start-up, handling of the capillary, filling of the capillary, placing the capillary in the cartridge, placing the test cartridge in the test device, duration of analysis and display of results.
Results
From May to June 2012, 100 children (56% boys) at a median age of 9.9 years (IQR 9.8) were tested and 35 adults (54% men) at a median age of 35.5 (IQR 16.2).
In children aged 0–18 years
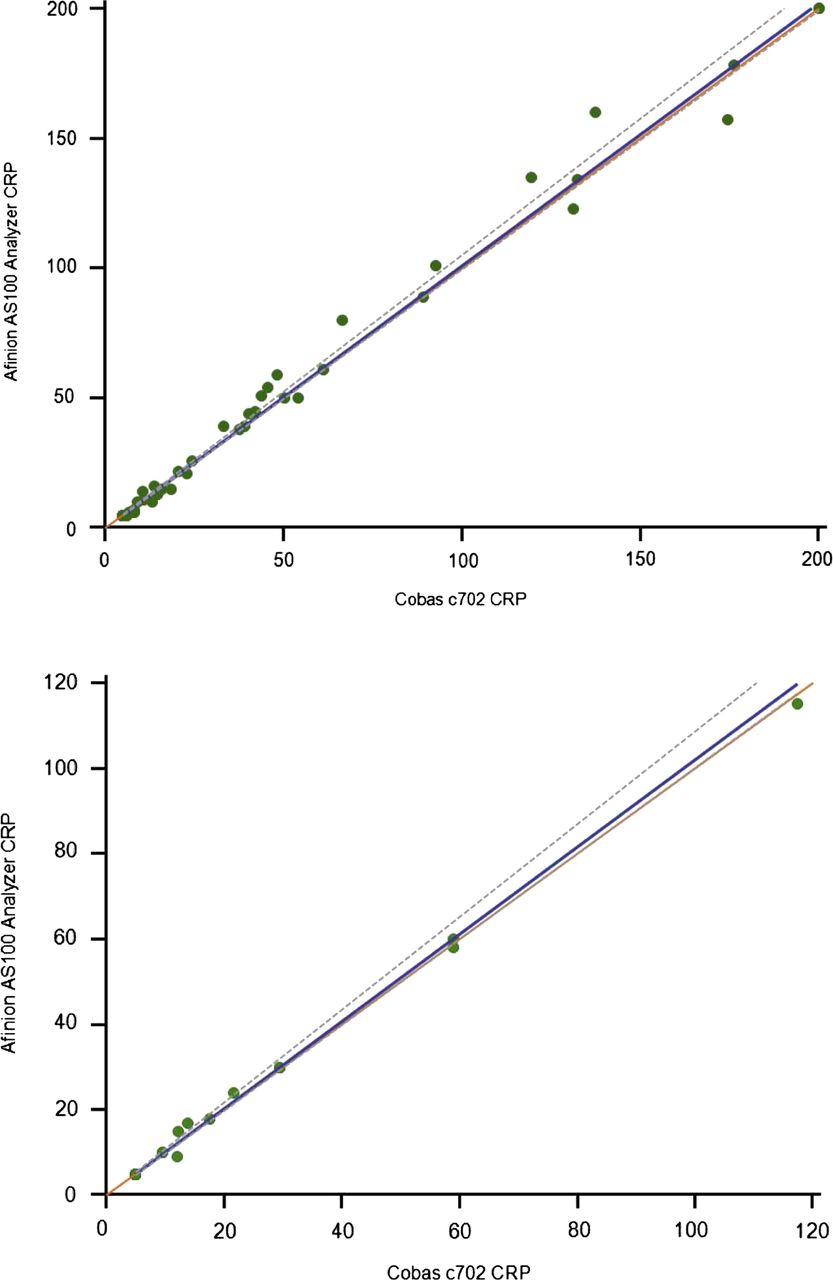
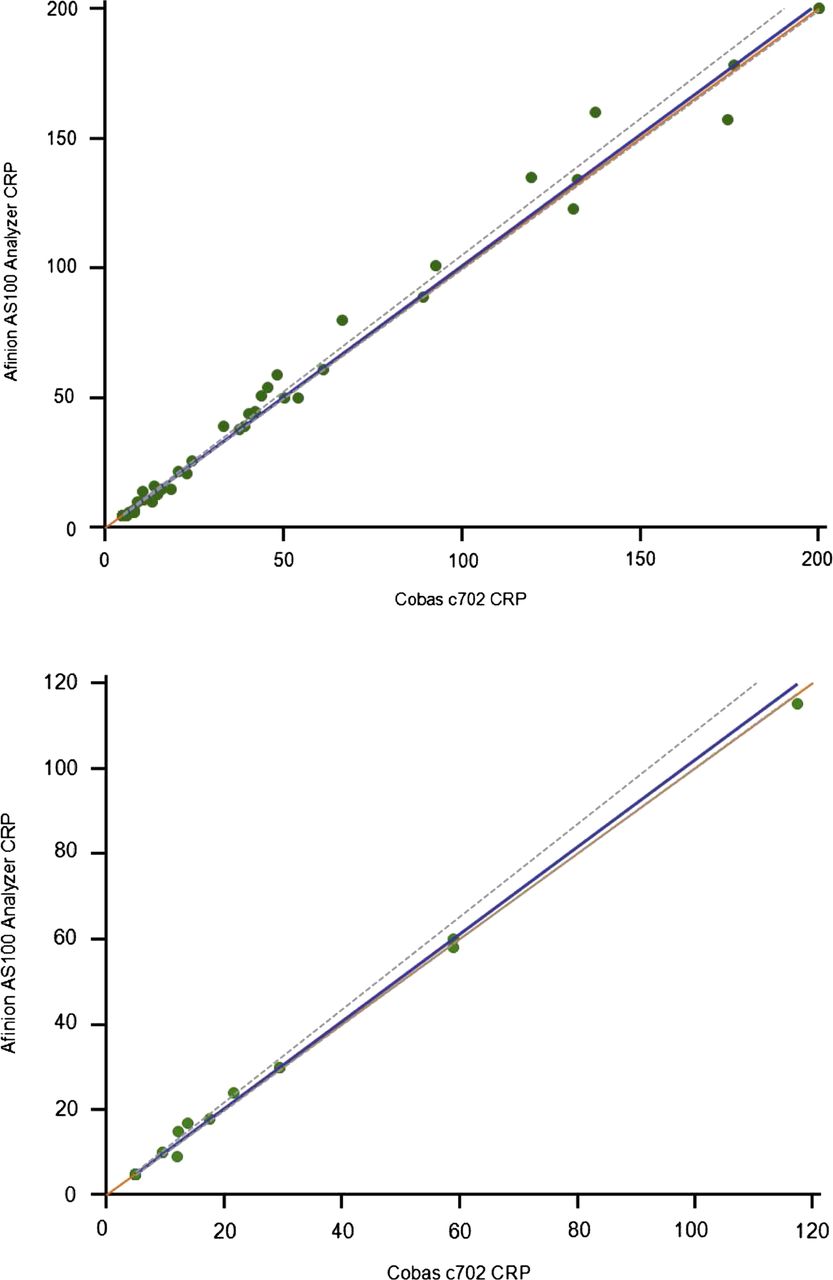
Figure 1 A illustrates the agreement on a Bland–Altman-plot in 100 children between the CRP test results on the Afinion AS100 Analyzer and the CRP test results on Cobas c702 with a mean difference of 0.1% with 95% limits of agreement from −17.6% to 17.4% with all differences below ±23 mg/L (figure 2A). A slope of 1.01 (95% CI 1.00 to 1.05) was found with perfect correlation (y=1.01x−0.04) even at high CRP concentrations (figure 3A).

(A) Percentage difference plot of the agreement between the Afinion point-of-care (POC) CRP test results on an AS100 Analyzer and the CRP test results on a Roche Cobas c702 in 100 children. (B) Percentage difference plot of the agreement between the Afinion POC CRP test results on an AS100 Analyzer and the CRP test results on a Roche Cobas c702 in 35 adults. CRP, C reactive protein; orange dots: scatter; cyan line: mean agreement between both methods; red line: 95% limits of agreement.

(A) Absolute difference plot of the agreement between the Afinion point-of-care (POC) CRP test results on an AS100 Analyzer and the CRP test results on a Roche Cobas c702 in 100 children. (B) Absolute difference plot of the agreement between the Afinion POC CRP test results on an AS100 Analyzer and the CRP test results on a Roche Cobas c702 in 35 adults. CRP, C reactive protein; orange dots: scatter; cyan line: mean agreement between both methods; red line: 95% limits of agreement.
{kind=link}
{kind=link}
{kind=link}
(A) Correlation between the Afinion point-of-care (POC) CRP test results on an AS100 Analyzer and the CRP test results on a Roche Cobas c702 in 100 children. (B) Correlation between the Afinion POC CRP test results on an AS100 Analyzer and the CRP test results on a Roche Cobas c702 in 35 adults. CRP, C reactive protein; green dots: scatter; blue line: regression line; grey dotted line: 95% CIs of regression; orange line: y=x.
In adults aged 18–65 years
Figure 1B shows a mean difference of 1.3% with 95% limits of agreement from −15.4% to 12.8% in the 35 adults with all differences below ±4 mg/L (figure 2B). A slope of 1.02 (95% CI 1.01 to 1.08) was found with perfect correlation (y=1.02x−0.10) (figure 3B).
User-friendliness of the POC CRP device
The results of the survey provided median scores of 4–5 for all items evaluated.
Discussion
We were able to confirm the analytical accuracy of the Afinion POC CRP test in comparison with an immunoturbidimetric CRP test on a Cobas c702 device in children as well as in adults. Even at high CRP concentrations, the test demonstrated high agreement and precise measurements. The few differences between both methods in cases with low CRP levels were not found to be clinically significant, as they would not change decisions on further treatment or testing. All participating physicians and the principal investigators deemed the device user-friendly.
This is the first study to examine the Afinion CRP test in children. We performed capillary blood CRP tests in a large sample of 100 children. A total of 100 of the 104 children (and their parents) eligible for inclusion were willing to participate, ensuring a representative sample of those children admitted to or attending a paediatric clinic. Although we provided a sufficiently large sample of children, generalisability to other settings (eg, primary care) and populations (eg, neonates) cannot be guaranteed.
As this is the first study to evaluate the Afinion CRP test, we can only compare these findings with those of the Nycocard, its predecessor. Previous studies have confirmed its use to be acceptable in children.5–8 It, however, required additional steps such as dilution of the sample, applying a conjugate, washing the sample and finally reading the test result. We believe the Afinion CRP Analyzer to be undeniably user-friendlier as confirmed by our results.
Diagnostic accuracy studies are needed to evaluate the added value of POC CRP tests in diagnosing serious infections in children. The selected device met primary requirements to assess an acutely ill child at risk of a serious infection. Further research is needed to support this assumption.
Conclusions
In this study, the Afinion AS100 Analyzer was accurate in children and should be considered reliable and user-friendly.
Acknowledgments
We would like to thank Professor Dr Christel Van Geet, Professor Dr François Vermeulen, the nursing staff of Wards 302 and 341 of the Department of Pediatrics, University Hospitals Leuven and all participating physicians for contribution to the study and data collection. We would like to thank Professor Flor Vanstapel and Professor Els Dequeker for their advice on point-of-care testing and laboratory testing of C reactive protein. We would also like to thank Alere Health bvba, Belgium, for providing the point-of-care devices and the technical support. We would like to thank all the children and parents who participated in this study.
Footnotes
-
Competing interests DMAB is a recipient of a senior clinical investigator fellowship from the Fund for Scientific Research (FWO) Flanders.
-
Ethics approval Ethical Review Board of the KU Leuven, Belgium.
-
Provenance and peer review Not commissioned; externally peer reviewed.