Article Text

Abstract
Background Chronic respiratory diseases (CRD) are common, are increasing in prevalence, and cause significant morbidity and mortality worldwide. However, we have limited knowledge on causes of death of patients with CRD in the general population.
Objective We evaluated mortality rates and causes of death over time in patients with CRD.
Methods We used linked primary care and mortality data to determine mortality rates and the most common causes of death in people with CRD (including asthma, bronchiectasis, COPD and interstitial lung diseases (ILD)) during 2005–2015 in England.
Results We identified 558 888 patients with CRD (451 830 asthma, 137 709 COPD, 19 374 bronchiectasis, 10 745 ILD). The age-standardised mortality rate of patients with CRD was 1607 per 100 000 persons (asthma=856, COPD=1503, ILD=2609, bronchiectasis=1463). CRD mortality was overall 54% higher than the general population. A third of patients with CRD died from respiratory-related causes. Respiratory-related mortality was constant, while cardiovascular-related mortality decreased significantly over time. COPD accounted for the majority of respiratory-related deaths (66% overall) in all patient groups except ILD.
Conclusions Patients with CRD continue to experience substantial morbidity and mortality due to respiratory diseases. Disease-modifying intervention strategies are needed to improve outcomes for patients with CRD.
- copd epidemiology
- asthma epidemiology
- bronchiectasis
- clinical epidemiology
Statistics from Altmetric.com
Key Messages
What is the key question?
What do patients with chronic respiratory diseases (asthma, bronchiectasis, COPD, interstitial lung disease) die from and how have mortality rates changed?
What is the bottom line?
Having a CRD carries a high mortality risk, except in asthma. In patients with CRD, there has been no improvement in death from respiratory causes.
Why read on?
This is the largest observational study of patients with chronic respiratory disease.
Introduction
Chronic respiratory diseases (CRDs) including asthma, bronchiectasis, COPD and interstitial lung diseases (ILDs) are common, are increasing in prevalence, and cause significant morbidity and mortality worldwide.1–4 Despite declines in CRD mortality in some specific populations in recent years, there has been an overall increase of 30% in CRD mortality in the general population since 1980.5 With an ageing population, improvements in treatments and earlier diagnosis, it is not known whether there have been changes in the underlying causes of death in patients with CRD over time.
Lung diseases are responsible for 20% of all deaths in the UK, most due to lung cancer, COPD and pneumonia.6 The UK has the highest respiratory mortality rate in the Organisation for Economic Co-operation and Development.7 8 While mortality rates for cardiovascular disease (CVD) in the general population have fallen in recent years, mortality due to lung diseases has remained constant.6 These rates have not previously been estimated among patients diagnosed with a CRD.
Asthma is a highly prevalent global disease,4 yet there is limited knowledge on the cause of death. Within developed countries, asthma-specific mortality (from acute asthma attacks) has steadily declined over the past few decades,9 but far less is known about all-cause asthma mortality. The only comprehensive study to address this question, between 1999 and 2008, in a Canadian provincial health administrative database, found that patients with asthma had a lower mortality rate than the general population, and were most likely to die from other comorbid disorders than their asthma.10
Bronchiectasis is a burden in many countries, including the UK, though comprehensive global data remain elusive.11–13 Few previous studies have looked at rates and causes of death in patients with bronchiectasis.13 14
COPD prevalence and mortality has increased globally since 1990 and carries an especially high disease burden in low-income and middle-income countries.4 15 COPD itself is a major cause of mortality for patients with COPD, along with other respiratory diseases and cancer; it has been reported that a third of patients with COPD die from CVD.16–19
Few studies investigate ILD as a whole; many studies focus on idiopathic pulmonary fibrosis (IPF), pulmonary sarcoidosis and pneumoconiosis separately. While the incidence of and mortality due to IPF is known to be increasing worldwide and in the UK,20–23 there is a paucity of data on incidence and mortality in patients with sarcoidosis and pneumoconiosis.5 23
Many studies have investigated respiratory deaths reported on death certificates;4 6 17 however, relying on death certificates alone means that a large number of patients with CRD are missed. Previous studies have found that anywhere between 6% and 82% of patients with CRD have a CRD listed anywhere on their death certificate.14 21 24 25
The aims of this study were to calculate the all-cause and disease-specific mortality rates of patients with CRD, including patients with asthma, bronchiectasis, COPD and ILD, compared with the general population, as well as to investigate the temporal pattern of causes of death between 2005 and 2015.
Methods
Data sources
Primary care electronic healthcare records from the Clinical Practice Research Datalink (CPRD), the largest validated anonymised source of longitudinal health data including demographic, medical diagnosis, prescription and laboratory test data that has been shown to be representative of the UK population.26 27 Mortality and population size data from the Office of National Statistics (ONS) for England and Wales.28 29 Socioeconomic status (SES) measured in relation to patients’ postcodes from the Index of Multiple Deprivation (IMD)30.
Study population
Patients over the age of 18 years with asthma, bronchiectasis or ILD, and patients over the age of 35 years with COPD,31 identified in CPRD using prespecified Read codes, and alive at any time between 1 January 2004 and 31 December 2015, were included. Patients were considered eligible if they were registered with a practice that consents to participate in the record linkage scheme. Follow-up began at the latest of the following dates: study start date, the patient’s eighteenth birthday, the date CPRD deemed the submitting general practice was ‘up to standard’ (ie, the practice had passed a number of quality checks and was deemed suitable for research use), the date a patient joined the practice or the date of first diagnosis with CRD. Patients were considered to have asthma at the time of death if their most recent asthma code was within 3 years of their death to distinguish between resolved and current disease32.
Exposure
CRD diagnosis: asthma, bronchiectasis, COPD or ILD. A validated code list was used to identify patients with asthma.33 A validated COPD code list34 was the basis of our COPD code list (see online supplement for additional codes). The code lists used to identify patients with bronchiectasis12 and ILD35 are published.
Supplementary file 1
Outcome
Mortality rate and underlying cause of death from ONS. ONS derives underlying cause of death using standardised guidelines from information available on death certificates and coded using the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10)36.
Covariates
Age was measured in years. SES from IMD 2015 data divided into quintiles, where 1- is most deprived.30 Baseline body mass index (BMI; kg/m²) was classified as ‘underweight’ (<18.5), ‘healthy weight’ (18.5–24.9), ‘overweight’ (25.0–29.9), and ‘obese’ (>30.0). Baseline smoking status was classified as ‘never smoker/not recorded’, ‘current smoker’ and ‘former smoker’.12
Statistical analyses
All statistical analyses were performed in STATA V.15 (StataCorp, College Station, Texas, USA).
Mortality rates
Using linked CPRD and ONS mortality data, we analysed mortality trends from 2005 to 2015 among people with each CRD. We calculated comparative mortality rates in men and women with each CRD in England to mortality rates in the general population from ONS data. We calculated the crude all-cause mortality rates by calculating the number of deaths in people with each CRD in the CPRD data set and dividing by the midpoint CRD population for that year, then averaging over the 10-year study period. Additionally we calculated mortality figures stratified by age, sex, BMI, smoking status and SES.28 29 We then calculated age-standardised (using the 2013 European Standard Population) mortality. We compared our results to the ONS published data on adult all-cause mortality figures.
Changes in causes of mortality
We investigated all-cause mortality and disease-specific mortality and determined proportions of deaths due to specific causes in people with each CRD using the ONS-derived underlying cause of death. Trends in cause of death were assessed using χ2 tests.
Sensitivity analyses
As a sensitivity analysis, we computed trends in causes of death using both ONS-derived underlying cause of death and the cause of death as reported in the first position on the death certificate, which may be ill-defined.37 Sensitivity analyses in each of the disease populations was undertaken by examining mortality rates and causes of death after excluding patients that had a co-diagnosis of another CRD.
Results
Cohort characteristics
We identified 558 888 patients with CRD who met the inclusion and exclusion criteria (figure 1; online supplementary material S1), of whom 75 789 died (14%) between 2005 and 2015 (table 1). Average age at death increased from 77.4 years (95% CI 77.2 to 77.8) in 2005 to 79.2 years (95% CI 78.9 to 79.4) in 2015.

Flow chart of patient inclusion. CRD includes asthma, bronchiectasis, COPD and ILD. Disease component numbers do not sum up to total numbers as patients were able to be part of multiple disease groups. CPRD, Clinical Practice Research Datalink; CRD, chronic respiratory disease; ILD, interstitial lung disease; ONS, Office of National Statistics.
Descriptive statistics of deaths of patients with chronic respiratory disease (CRD)
Mortality rates
The cumulative crude all-cause mortality rate for patients with CRD between 2010 and 2015 was 3030 per 100 000 patients (95% CI 3022 to 3038) (table 2), with a rate of 0.809 per 100 000 person-years (95% CI 0.807 to 0.811). Crude rates were higher in men, older age groups and current smokers (online supplementary material S2), as well as among patients with lower BMI and those living in the least deprived areas (online supplementary material S3). Age standardised mortality rates (ASMR) increased from 1332 per 100 000 (95% CI 1328 to 1335) in 2005 to 2673 per 100 000 (95% CI 2666 to 2680) in 2015 (figure 2). ASMR among patients with CRD was 54% (95% CI 44% to 64%) higher than the general population and was higher after excluding patients with comorbid CRD (online supplementary material S4).
Mortality rates stratified by CRD, 2004–2015

Age-standardised mortality (ASM) per 100 000 population compared with the general population, 2005–2015. Presented for all patients with asthma, bronchiectasis, COPD and interstitial lung disease (ILD). Rates compared with the general population. Groups differentiated as ‘only’ refer to those patients with that respiratory disease and no other respiratory disease comorbidities. Disease groups presented are mutually exclusive. CRD, chronic respiratory disease; pop, population.
Cause of death
Of the individuals 32 664 (43%) had a record of their underlying diagnosed lung disease mentioned as one of the causes of death on their death certificates. The leading causes of death among all patients with CRD were diseases of the respiratory system (32%) (figure 3; online supplementary material S1), where deaths due to COPD and pneumonia accounted for 79% of all respiratory deaths (table 3). The second most common cause of death was diseases of the circulatory system (26%) (table 3; figure 3; S5). Neoplasms (24%) were the third leading cause of death (figure 3; online supplementary material S5), with lung cancer accounting for over a third of cancer deaths (table 3). The other main causes were mental and behavioural disorders/diseases of the nervous system (6%) and diseases of the digestive system (4%) (figure 3; online supplementary material S1). Results were consistent in our sensitivity analyses excluding patients with comorbid respiratory diseases (online supplementary material S6) and analysing causes of death as listed in the first position on death certificates (supplementary material S7).

Leading causes of death among patients with chronic respiratory disease (CRD) by disease. Presented as percentages of all deaths per year for the overall CRD and by individual disease; including asthma, bronchiectasis, COPD and interstitial lung disease (ILD). International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) chapters F (mental and behavioural disorders) and G (diseases of the nervous system) have been combined. ‘Other’ refers to causes of death categorised in all ICD-10 chapters outside of C, D00–48, F, G, I, J and K.
Five leading causes of death by underlying CRD
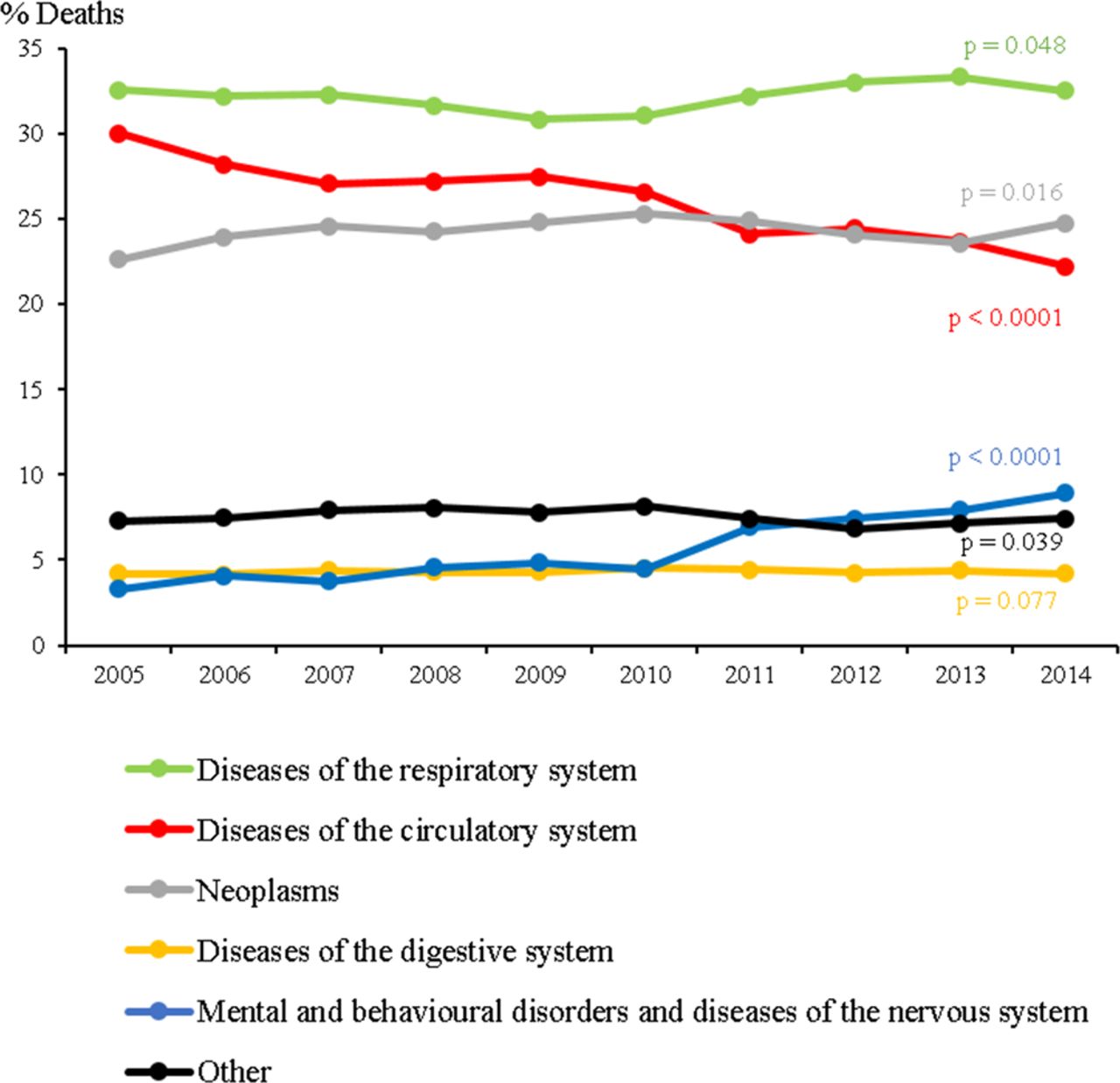
The proportion of deaths due to respiratory diseases remained steady in the CRD population as a whole, and by individual disease, from 2005 to 2015 (p-trend >0.05) (figure 4; online supplementary material S8). A significant decrease in the proportion of deaths attributed to circulatory disease was seen in the CRD population as a whole, from 30% in 2005 to 23% in 2015 (figure 4), and by each individual disease population (online supplementary material S8). Among patients with asthma, a small decrease in the proportion of respiratory-related deaths was seen over time, in keeping with the increase in the proportion of mental disorders (online supplementary material S8). And after considering the age distribution of the population (online supplementary material S9) these trends were most prominent among the older age groups.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Trends in leading causes of death in the chronic respiratory disease (CRD) population, 2005–2015. Presented as % of all deaths per year for the overall CRD population; including asthma, bronchiectasis, COPD and interstitial lung disease (ILD). ICD-10 chapters F (mental and behavioural disorders) and G (diseases of the nervous system) have been combined. ‘Other’ refers to causes of death categorised in all ICD-10 chapters outside of C, D00-48, F, G, I, J and K. Significant p values (α <0.05) from χ2 test for trend are shown.
Discussion
This is the first and largest study to use an unselected cohort (ie, non-trial population) of patients with CRD (asthma, bronchiectasis, COPD and ILD) diagnosed from their primary care records to assess causes of mortality over a 10-year period. Mortality was lowest among patients with asthma, in keeping with the general population, but remained high among patients with bronchiectasis, COPD and ILD. Over a third of deaths were attributed to respiratory diseases while a significant decrease in deaths attributed to CVD was observed.
Mortality in patients with CRD
Compared with the general population, patients with CRD experienced a 54% higher mortality overall. Only 43% of all patients with CRD had their underlying respiratory disease mentioned anywhere on their death certificate. Patients with CRD were more likely to die from neoplasms or respiratory illness, but less likely to die of CVD, than they were 10 years ago. Over this period, improvements in comorbid disease management, risk stratification and new medications have driven this reduction in CVD deaths, as reflected in the general population.38 Cancer continued to be attributed to a significant proportion of the causes of death among the CRD population, despite a decline in the general population.39 Increased numbers of deaths due to mental and behavioural disorders and diseases of the nervous system are likely explained by the ageing population and increased detection, particularly observed after the cause of death coding changes in 201040.
Mortality in patients with asthma
Patients with asthma, those without other respiratory diagnoses, experienced lower all-cause mortality rates compared with the general population. Patients with asthma with other respiratory diseases experienced high but decreasing all-cause mortality due to the inclusion of comorbid COPD and patients with a history of smoking suggesting possible improvements as awareness of overlap syndromes has increased over time. The most common causes of death in all patients with asthma were COPD and ischaemic heart disease. After excluding patients with other diagnosed respiratory diseases, COPD remained among the leading causes of respiratory-related deaths. This could be due to misdiagnosis, related to difficulty in distinguishing clinically between asthma and COPD, or possibly misclassification of the underlying cause of death41 42.
Mortality in patients with bronchiectasis
We observed higher ASMR among patients with bronchiectasis compared with a previous UK study;13 these rates increased after including patients with other CRDs. Patients with bronchiectasis were most likely to die from bronchiectasis, ischaemic heart disease and ‘other’ cancers; similar to previous research.12 Earlier detection of bronchiectasis with effective management of exacerbations and reductions in exacerbation frequency may decrease excess mortality.
Mortality in patients with COPD
Mortality remained high among patients with COPD, similar to previous UK reports,37 43 but did not reflect the decrease presented in previous global estimates.4 Despite advances in the management of COPD, introduction of new therapies, and the publication of new guidelines and strategies31 44–46, a third of deaths among patients with COPD are still attributed to non-malignant respiratory diseases, mostly COPD, in keeping with previous clinical trial data.47 Just over a quarter of deaths of patients with COPD were attributed to CVD, less than the a third of deaths previously reported,16–19 and possibly related to earlier recognition and better management of CVD in the past decade. These results highlight the lack of treatments that reduce respiratory-related mortality and the need to pair early diagnosis with effective disease-modifying interventions48.
Mortality in patients with ILD
Patients with ILD experienced increasing high mortality over the study period suggesting increasing incidence or increasing case ascertainment of these diseases.49 This further evidences the typically late stage of ILD at diagnosis resulting in poorer prognoses.23 50 The leading cause of death among patients with ILD remained their underlying lung disease, despite being at increased risk for CVD.35 The increasing availability of antifibrotic therapies may change this trend in the future51.
Strengths
This study used linked primary care and mortality data to assess cause of death in patients with CRD. Previous studies investigating CRD deaths identified patients as those for whom CRD was recorded on their death certificate or who were hospitalised.8 17 21 52 53 Relying on death certificates alone means that a large number of patients with CRD may be missed, as previous studies have found that anywhere between 6% and 82% of patients with CRD have a CRD listed anywhere on their death certificate, consistent with the 43% we observed.21 24 25 This is the first and largest observational study to estimate mortality rates and causes over time using a nationally representative cohort of patients with CRD.
Another strength of this study is that ONS is nearly 100% complete, with a large proportion of registered deaths certified by a medical practitioner, and an ever-increasing accuracy of recordings.40 Since 1993, automated coding has been in place for cause of death with application of WHO rules allowing international comparisons.54 While the accuracy of the underlying cause provided by ONS, which is a derived variable, relies on correct recording of all contributing causes of death55, in a review undertaken by ONS, the proposed and medical examiner confirmed underlying cause of death matched at ICD chapter level in 88% of cases and there was exact agreement (to four digits) in 78% of cases, rising to 80% when records matching to three digits were included.56 Furthermore, our sensitivity analysis comparing the ONS-derived underlying cause of death to the first listed cause of death on the death certificate did not significantly change the proportions of leading causes of death, suggesting that the algorithm used to derived cause of death is sufficiently accurate.
Limitations
One potential limitation of studies using electronic healthcare records is the validity of case definitions. For asthma and COPD we used previously validated definitions,33 34 but there are no validated definitions for ILD and bronchiectasis. However, ILD and bronchiectasis diagnoses are made in a secondary care setting and are confirmed by CT; it is unlikely that diagnoses of either ILD or bronchiectasis will be recorded within primary care without confirmation from secondary care. It is well recognised, as found in our study too, that there is a large proportion of patients with overlapping diagnosis of asthma, COPD and bronchiectasis. Our inclusion of these patients reflects clinical practice and explains the large proportion of respiratory deaths attributed to COPD.
We were not able to compare mortality rates using person-time of disease as data for the general population were obtained via publicly available ONS mortality reports. Therefore morality should be interpreted taking into account that duration of disease was not included in estimating mortality rates. In addition we did not include details on disease severity or use of medications which may have an impact on overall survival. Future research should investigate disease phenotypes with use of interventions to evaluate whether the excess risk of mortality we observed is modifiable. Where data were missing in the CRD cohort, categories were either considered missing at random or grouped where the number of missing information was low. However there is a possibility that we may have misclassified patients.
Conclusions
This is the largest and most contemporary study to investigate the mortality of patients with CRD using a nationally representative UK population. All-cause mortality remains high in people with CRD, in contrast to the general population. Disease-modifying intervention strategies are needed to improve CRD survival.
Acknowledgments
The authors thank Miss Navdeep Bual for assisting in the compilation of the descriptive statistics provided in the supplement tables.
References
Footnotes
AVG and ELA contributed equally.
Contributors ELA defined the cohort. AVG determined cause of death. AVG and ELA performed the statistical analyses and drafted the original manuscript. CIB, VN and JKQ reviewed the analyses. JKQ designed the study. All authors took part in the production of the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests AVG is supported by an educational grant and is an employee of Boehringer Ingelheim Ltd. JKQ’s research group has received funding from MRC, Wellcome Trust, BLF, GSK, Insmed, AZ, Bayer and BI for other projects, none of which relate to this work. JKQ has received funds from AZ, GSK, Chiesi, Teva and BI for Advisory board participation or travel. VN is an NIHR clinical lecturer.
Ethics approval The protocol for this research was approved by the Independent Scientific Advisory Committee (ISAC) for MHRA Database Research (protocol number 17_086R) and the approved protocol was made available to the journal and reviewers during peer review. Generic ethical approval for observational research using the CPRD with approval from ISAC has been granted by a Health Research Authority (HRA) Research Ethics Committee (East Midlands – Derby, REC reference number 05/MRE04/87). Following ethics approval by ISAC, the study population was expanded to include all adults, 18 years of age and older, to be in line with most studies in this research area; and IPF was expanded to ILD, to better understand the burden of CRD in the UK. These were considered minor amendments and did not require further ISAC approval. Linked pseudonymised data were provided for this study by CPRD. Data are linked by NHS Digital, the statutory trusted third party for linking data, using identifiable data held only by NHS Digital. Select general practices consent to this process at a practice level with individual patients having the right to opt out.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement Data are available on request from the CPRD. Their provision requires the purchase of a license, and our license does not permit us to make them publicly available to all. We used data from the version collected in October 2017 and have clearly specified the data selected in our Methods section. To allow identical data to be obtained by others, via the purchase of a license, we will provide the code lists on request. Licences are available from the CPRD (http://www.cprd.com): The Clinical Practice Research Datalink Group, The Medicines and Healthcare products Regulatory Agency, 5th Floor, 151 Buckingham Palace Road, Victoria, London SW1 W 9SZ.
Patient consent for publication Not required.
Linked Articles
- Airwaves