Article Text

Abstract
Objective Current clinical practice guidelines advocate shared decision-making (SDM) in prosthetic valve selection. This study assesses among adult patients accepted for aortic valve replacement (AVR): (1) experience with current clinical decision-making regarding prosthetic valve selection, (2) preferences for SDM and risk presentation and (3) prosthetic valve knowledge and numeracy.
Methods In a prospective multicentre cohort study, AVR patients were surveyed preoperatively and 3 months postoperatively.
Results 132 patients (89 males/43 females; mean age 67 years (range 23–86)) responded preoperatively. Decisional conflict was observed in 56% of patients, and in 25% to such an extent that it made them feel unsure about the decision. 68% wanted to be involved in decision-making, whereas 53% agreed that they actually were. 69% were able to answer three basic knowledge questions concerning prosthetic valves correctly. 56% were able to answer three basic numeracy questions correctly. Three months postsurgery, 90% (n=110) were satisfied with their aortic valve prosthesis, with no difference between mechanical and bioprosthetic valve recipients.
Conclusions In current clinical practice, many AVR patients experience decisional conflict and suboptimal involvement in prosthetic valve selection, and exhibit impaired knowledge concerning prosthetic valves and numeracy. Given the broad support for SDM among AVR patients and the obvious need for understandable information, to-be-developed tools to support SDM in the setting of prosthetic valve selection will help to improve quality of decision-making, better inform and actively involve patients, and reduce decisional conflict.
Trial registration number NTR3618.
- QUALITY OF CARE AND OUTCOMES
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Shared decision-making (SDM) receives more and more attention in healthcare. Prosthetic aortic valve selection concerns a value sensitive decision. The 2014 ACC/AHA Valvular Heart Disease Guidelines and 2012 ESC/EACTS guidelines highlight the importance of SDM.
What does this study add?
However, the attitude of patients towards SDM in prosthetic aortic valve selection remains unexplored. Therefore, we conducted a prospective multicentre cohort study among elective adult aortic valve replacement (AVR) patients.
How might this impact on clinical practice?
We are convinced that our observations provide an important information base on which we can build effective tools for the implementation of SDM in prosthetic aortic valve selection. This will result in better informed patients who feel more responsible for their own health and disease management, and it will hopefully lead to better informed decision-making and better quality of care.
Introduction
For most patients who require aortic valve replacement (AVR), two options exist: mechanical or bioprosthetic valve replacement. Each prosthetic valve has specific risks and benefits. Mechanical valves are thrombogenic and therefore require lifelong anticoagulation. Bioprosthetic valves carry a higher risk of reoperation due to valve degeneration.1 ,2 There is no apparent difference in survival for adult patients with a mechanical or bioprosthetic valve.3 ,4 Therefore, prosthetic valve choice is mainly driven by valve-specific risks and benefits. Given the different nature of these risks and benefits for mechanical and bioprosthetic valves, informed patient preferences deserve consideration in decision-making.
The 2014 ACC/AHA Valvular Heart Disease Guidelines state that prosthetic valve choice should be a shared decision process,2 while the 2012 ESC/EACTS guidelines highlight the importance of considering informed patient preferences (Class 1 recommendations).1 We previously showed that the majority of the Dutch cardiothoracic surgeons and cardiologists are of the opinion that prosthetic aortic valve selection should ideally be done together with the patient and they report to communicate to the patient most important risks of the different prosthetic valve types. Nevertheless, only half of them actively involves patients in prosthetic valve selection.5 Although the guidelines advocate shared decision-making (SDM), clinicians do not have any tools to engage this activity.
In order to engage in SDM, both the clinician and the patient should be able and willing to participate. It is unknown how patients experience decision-making in prosthetic aortic valve selection and what their attitude is towards SDM. The purpose of this prospective study was to assess among adult patients accepted for AVR: (1) experience with current clinical decision-making regarding prosthetic valve selection, (2) preferences for SDM and risk presentation and (3) prosthetic valve knowledge and numeracy.
Methods
This study was approved by the institutional review board of all three participating centres (Erasmus MC MEC nr. 12-323). Written informed consent was obtained. Participants were adult patients who were accepted for elective AVR in one of the three hospitals between September 2012 and June 2013. Patients had to be legally capable. Two surveys were conducted, one preoperatively after preoperative outpatient counselling, and another 3 months postoperatively.
Preoperative survey
Patient experience with prosthetic valve selection
Multiple choice (MC) questions assessed which clinician (surgeon, cardiologist, both or other) performed the preoperative consultation with regard to prosthetic valve choice, if a friend or family member was involved in prosthetic valve choice, patient opinion on the amount of time available for prosthetic valve choice, and how patients valued their participation in prosthetic valve choice.
The Decisional Conflict Scale (DCS) was used to measure the degree of uncertainty about which course of action to take and the main modifiable factors contributing to uncertainty. It is a 16-item questionnaire with five subscales: uncertainty, informed, values clarity, support and effective decision. Total scores <25 are associated with no decisional conflict and implementation of decision. Scores exceeding 25 are associated with decisional conflict, with higher scores indicating higher decisional conflict. Scores ≥37.5 are associated with decision delay or feeling unsure about implementation.6
A 1–5 Likert scale was used to assess how patients value the importance of the different risks and benefits associated with a mechanical and bioprosthetic valve.
Patient preferences for SDM and risk presentation
A 1–5 Likert scale and a Control Preferences scale were used to assess patient view on participation in decision-making.7
Patient preference for presentation of scientific evidence was assessed by asking patients to rate four graphical formats of scientific evidence: a horizontal bar, pie chart and two pictographs (a visual presentation of data).8
Patient prosthetic valve knowledge and numeracy
Information that patients perceived from the treating physician with regard to prosthetic valve selection and patient knowledge regarding the risks and benefits associated with mechanical and bioprosthetic valves was assessed by MC questions and a 1–5 Likert scale.
Patient numeracy was assessed using the Numeracy Scale.9
For a detailed description of the preoperative survey, see online supplementary appendix 1.
Postoperative survey
Patient experience with prosthetic valve selection
MC questions and a 1–5 Likert scale were used to assess patient opinion on the amount of time available for prosthetic valve choice, how patients value their participation in prosthetic valve choice, and patient satisfaction with the type of prosthetic valve they received.
Valve-specific quality of life (QoL) was measured with a valve-specific questionnaire.10
Patient preferences for SDM
Patient view on participation in decision-making was assessed by a 1–5 Likert scale and a Control Preferences scale.
Patient prosthetic valve knowledge
Information that patients perceived from the treating physician with regard to prosthetic valve selection was assessed with MC questions and a 1–5 Likert scale.
For a detailed description of the postoperative survey, see online supplementary appendix 2.
Statistical methods
Continuous variables were displayed by the mean, SD and range. Discrete variables were displayed as counts or proportions. Multiple imputations (5 iterations) were used to impute missing DCS values. To compare DCS group responses, the Mann–Whitney U test or Kruskal-Wallis test was used. To compare group responses between patients with a mechanical and bioprosthetic valve, the Mann–Whitney U test or Fisher exact test was used. Patients were allocated to the mechanical or bioprosthetic subgroup according to their survey answer. To compare group responses presurgery and postsurgery, the Wilcoxon signed-rank test was used. All tests were two-sided, and a p value of 0.05 or less was considered statistically significant. All statistical analyses were performed using IBM-SPSS V.20 (IBM Corp., Armonk, New York, USA).
Results
Preoperative survey
One hundred and thirty-two elective adult patients scheduled for AVR in three academic Dutch hospitals participated. Twenty-nine patients reported that they were to receive a mechanical valve, 74 a bioprosthetic valve, 2 a valve repair, and 29 did not know which valve they were going to receive. Table 1 displays patient characteristics. Patients with a bioprosthetic valve were significantly older than patients with a mechanical valve (p=0.000).
Patient characteristics
Patient experience with prosthetic valve selection
The preoperative consultation with regard to prosthetic valve choice was performed by the cardiologist (48%), the surgeon (18%), the surgeon and cardiologist together (16%) or other, for example a resident or physician assistant (19%). More than half of the patients (57%) involved a friend or family member in prosthetic valve choice. Sixty-four per cent of patients felt they had sufficient time to make a deliberate prosthetic valve choice and 64% felt they had a prosthetic valve choice.
Table 2 displays the results of the DCS.
Preoperative score on Decisional Conflict Scale (DCS)
There were no significant differences in the total DCS score between patients from the three different hospitals, and between patients with a mechanical versus bioprosthetic valve. The type of medical professional who performed the preoperative consultation did not influence the patient total DCS score. Patients who involved a friend or family member in prosthetic valve choice experienced significantly less decisional conflict than patients who made the decision alone (p=0.001).
Table 3 displays the patient's valuation of the importance of the different risks and benefits associated with mechanical and bioprosthetic valves.
Patient valuation of the importance of the different risks and benefits associated with a mechanical (MP) and bioprosthetic (BP) valve
Patient preferences for SDM and risk presentation
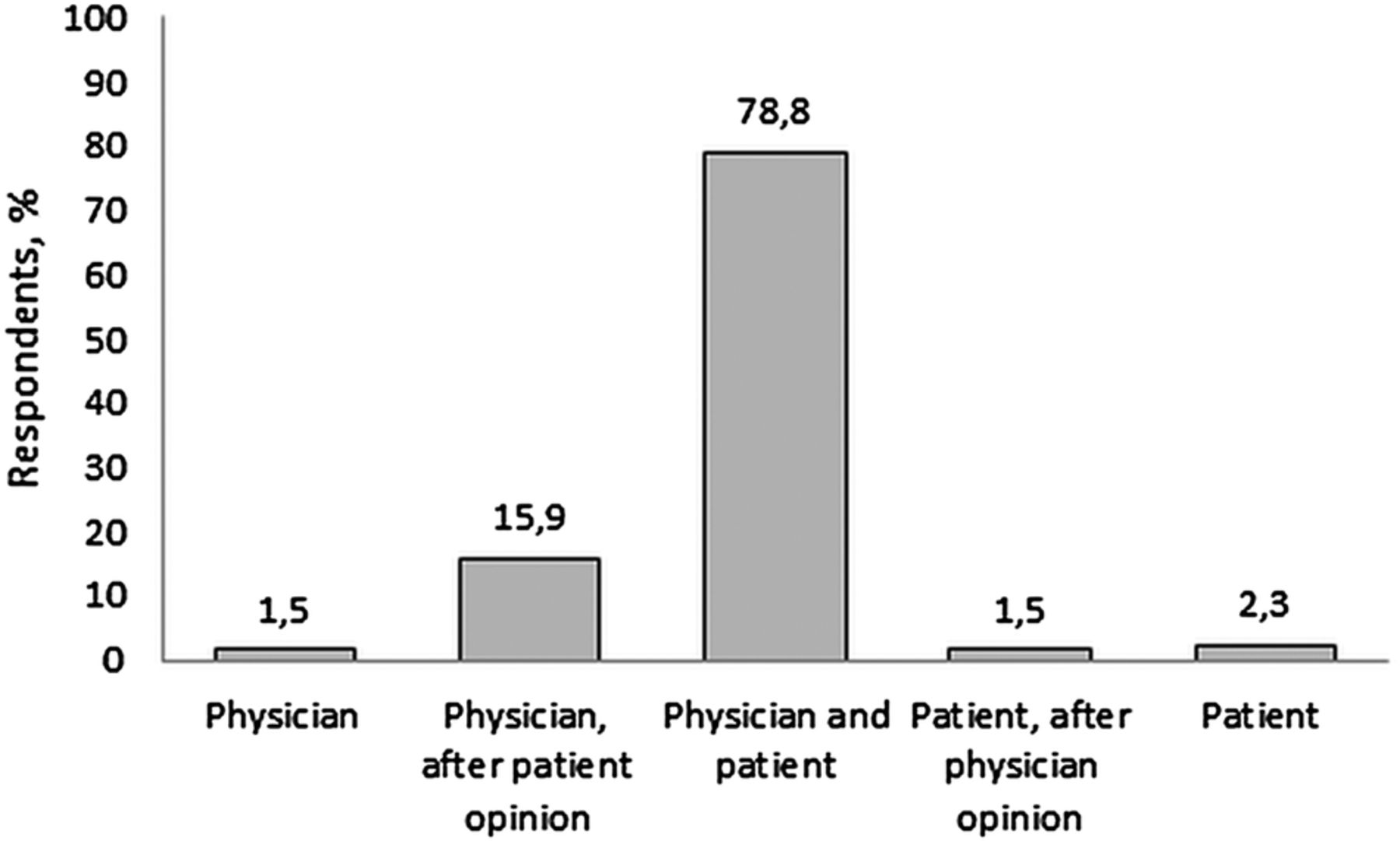
Patient preference for the final decision in prosthetic valve choice is displayed in figure 1. Sixty-eight per cent of patients wanted to be involved in decision-making, whereas 53% agreed that they were actually involved.
{kind=link}
Preoperative patient preference for final decision in prosthetic aortic valve choice (n=132).
The majority of patients (68%) preferred scientific evidence presentation in a pie chart, followed by the horizontal bar, and the two pictographs.
Patient prosthetic valve knowledge
Ninety-nine per cent of patients were aware that there are different types of aortic valve prostheses and 80% reported knowing which valve they were going to receive. Fifty-nine per cent were of the opinion that they had sufficient knowledge about the different types of aortic valve prostheses.
Table 4 displays patient prosthetic valve knowledge and numeracy.
Preoperative prosthetic valve knowledge and basic numeracy
Ninety-eight per cent of patients (n=129) answered all three questions concerning prosthetic valve knowledge. Of these, 5% were not able to answer any of the three questions correctly, 9% were able to answer one question correctly, and 16% and 69% were able to answer two and three questions correctly, respectively. There were no significant differences between patients with a mechanical and bioprosthetic valve. Sixty-four per cent of patients (n=84) answered all three numeracy questions. Four per cent were not able to answer any of the three questions correctly, 12% were able to answer one question correctly, 29% were able to answer two questions correctly and 56% were able to answer three questions correctly. There were no significant differences between patients with a mechanical and bioprosthetic valve.
Postoperative survey
One hundred and ten patients responded to the postoperative survey. Reasons for loss to follow-up included death (n=4), inability to complete the survey due to morbidity (n=5), cancelled operation due to comorbidity (n=2) or non-response (n=11). At the time of the postoperative survey, 86% of patients (n=95) were in NYHA class I or II, and 14% of patients (n=15) were in NYHA class III or IV. Twenty-eight patients reported that they received a mechanical valve, 81 a bioprosthetic valve and 1 a valve repair.
Patient experience with prosthetic valve selection
Seventy-seven per cent of patients felt they had sufficient time to make a deliberate prosthetic valve choice, which was significantly higher than preoperatively (p=0.001). Seventy-four per cent of patients felt they had a prosthetic valve choice (p=NS compared with preoperative).
Ninety per cent were satisfied with their valve prosthesis, 7% did not have an opinion and 4% were unsatisfied. There was no difference between patients with a mechanical and bioprosthetic valve.
The results of the valve-specific questionnaire are displayed in table 5.
Postoperative answers to a valve-specific questionnaire
Patient preferences for SDM
Eighty-seven per cent of patients wanted to be involved in decision-making, whereas 74% agreed that they were actually involved. This was significantly higher than preoperatively (68% vs 87%; p=0.000, and 53% vs 74%; p=0.000, respectively). Seventy-nine per cent preferred the final prosthetic valve choice to be a shared decision process (p=NS compared with preoperative).
Patient prosthetic valve knowledge
Ninety-nine per cent of patients were aware that there are different types of aortic valve prostheses and 100% reported knowing which valve they received. Seventy-four per cent were of the opinion that they had sufficient knowledge about the different types of aortic valve prostheses (p=NS compared with preoperative).
Discussion
In current Dutch cardiovascular clinical practice, patients who require AVR often experience decisional conflict and suboptimal involvement in prosthetic valve selection, and exhibit impaired numeracy. The majority of patients want to be involved in prosthetic valve selection, while only half of the patients actually feel involved. Given the limited patient knowledge of prosthetic valves and numeracy, there is an obvious need for improved information conveyance on prosthetic valve options and their associated risks and benefits.
Patient experience with prosthetic valve selection
The quality of decision-making does not appear to be influenced by the physician who discusses prosthetic valve selection, but our study results suggest that it is important for patients to involve a friend or relative, as this will reduce decisional conflict. This is in alignment with the 2014 ACC/AHA Valvular Heart Disease Guidelines that highlight the importance of involving family members in decision-making.2
Preoperatively, one-third of patients in this study felt they did not have sufficient time to make a deliberate prosthetic valve choice, and/or felt like they did not have a choice at all. This observation indicates room for improvement in decision-making, allowing for sufficient time and adequate information conveyance. Postoperatively, significantly more patients felt they had sufficient time than preoperatively. It is possible that preoperative stress may have influenced patient perception regarding the amount of time needed for prosthetic valve choice.
More than half of the patients experienced decisional conflict, and one in four patients to such an extent that it made them feel unsure about the decision. Decisional conflict was most evident in the uncertainty and values clarity subscales, suggesting that particular measures aimed at reducing patient uncertainty and improving value clarification will be effective in improving decision-making quality.6 Patient satisfaction with the selected prosthetic valve did not appear to be affected by the suboptimal decision-making. This may be caused by the phenomenon of choice closure: the process by which people come to perceive a decision to be resolved and complete. As choice closure results in greater satisfaction, it can explain at least in part why most patients were satisfied with their prosthetic valve.11
Preoperatively, the most common patient concerns about complications were related to the use of lifelong oral anticoagulation, the risk of bleeding or blood clot, valve sound and the need for a reoperation. Therefore, these topics require particular attention in the preoperative consultation. Interestingly, patients with a bioprosthetic valve more often answered ‘do not know’ when they were asked about complications. This may be due to their older age as it is known that older patients usually have a more passive role in decision-making and more difficulties understanding medical information.12 ,13
Patient preferences for SDM and risk presentation
A common misperception among clinicians is that many patients do not want to be involved in decision-making.14 The current study shows the contrary: most of the patients who require AVR do want to be involved. Previous studies in different medical fields also show that patients prefer to be involved in decision-making.15 ,16 In our study, more patients felt involved in decision-making postoperatively than preoperatively. The preoperative survey was conducted after preoperative outpatient counselling, on average 2 weeks before the operation. It is possible that patients received more information about prosthetic valve selection in the remaining time prior to and following the operation.
SDM receives more and more attention in healthcare. It can be described as a meeting of experts, the clinician as an expert on the medical issues and the patient as an expert on their values and preferences.14 SDM has several advantages, like increased patient knowledge, less patient anxiety, improved health outcomes, reductions in care and cost variation and more alignment of care with patient values.17 Therefore, it is not surprising that the 2014 ACC/AHA Valvular Heart Disease Guidelines and the 2012 ESC/EACTS guidelines state that SDM is a Class I recommendation for prosthetic valve selection.1 ,2 Nevertheless, despite the advantages of SDM and the fact that the guidelines advocate SDM, informed SDM is not often applied in daily clinical practice.18 ,19 SDM can be time-consuming and requires extra effort, which can be a barrier for cardiovascular professionals. In this respect, the use of a decision aid (DA) may be useful to support SDM. It has been shown that patients who use a DA have improved knowledge, more accurate risk perception, reduced decisional conflict and are more likely to receive care that is in line with their personal values.17 In the setting of prosthetic valve selection, a DA can inform patients about the different prosthetic valves and associated risks and benefits, help them clarify their preferences and guide them through the decision-making.
In order to participate in decision-making, patients should be able to understand what the available prosthetic valve options and their associated risks and benefits are. The way risks and benefits are presented influences the ability of the patient to understand the given information. Presenting statistical information in a graphical instead of numerical format increases people's understanding and may affect their decision-making.20 Previous studies show that a pictograph is the preferred option to present probabilistic information to patients.8 In this study, however, most patients preferred a pie chart. Of note, this study only investigated patient preference for the presentation of scientific evidence, while previous studies investigated which graph format achieved the best accuracy of risk perception. Therefore, although most patients in our study preferred a pie chart, this does not necessarily imply that it is the most effective way to communicate risks.
Patient prosthetic valve knowledge and numeracy
Almost half of the patients in our study felt that they had insufficient knowledge of prosthetic valves and almost one-third were unable to answer three basic knowledge questions about prosthetic valves correctly. We can only hypothesise that they either were not informed about the different prosthetic valves or received information that they were unable to comprehend. This observation nevertheless calls for the development of information provision on prosthetic valves that is tailored to the needs of patients.
Besides testing patient knowledge, we also deliberately tested numeracy. Since numbers are an inherent part of weighing risks and benefits,9 numeracy is of great influence on the capacity of patients to engage in SDM. One-third of the study patients did not answer any basic numeracy question. It could be that the questions were perceived too difficult and patients were afraid to answer them. Additionally, nearly half of the patients who did answer all numeracy questions exhibited impaired numeracy. These observations underline the importance of recognition among physicians that many patients have difficulties understanding numbers and need help in understanding the risks and benefits of treatment options.21
Given their limited basic knowledge regarding prosthetic valves and limited numeracy, many patients will experience difficulties in weighing the risks and benefits associated with mechanical and bioprosthetic valves. A DA with plain language, absolute risks presented as frequencies, and pictographs used to communicate risks and benefits20 may therefore be helpful in the setting of prosthetic valve selection. Building on this study and a previous survey concerning SDM in prosthetic valve selection among Dutch cardiovascular professionals,5 an information portal and DA for prosthetic valve selection has been developed and is currently being tested in a multicentre randomised controlled trial (RCT) to assess whether the use of the DA indeed improves the quality of decision-making and patient outcome in the setting of prosthetic valve selection.
Study limitations
This study population represents Dutch academic cardiovascular clinical practice. A limitation of the study was the relatively small sample size. Furthermore, surveys were completed at home and patients may have been influenced by family members or friends. Finally, it is possible that only the more motivated patients may have completed the questionnaire, which could introduce selection bias.
In conclusion, this study illustrates that in current Dutch cardiovascular practice, patients who require AVR experience suboptimal involvement in prosthetic valve selection, and exhibit impaired knowledge concerning prosthetic valves and numeracy. Given the broad support for SDM among patients and the cardiovascular community, and the obvious need for understandable information, implementation in clinical practice of the concept of SDM would be a major step forward in improving clinical decision-making in prosthetic valve selection. This will result in better patient involvement in decisions, increased patient knowledge, involvement and satisfaction and perhaps even a better QoL.
Acknowledgments
The authors would like to thank all the patients who participated in this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online supplement
Footnotes
Competing interests None.
Ethics approval Erasmus MC.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.