Article Text

Abstract
Urine samples are commonly collected from young children to diagnose or exclude urinary tract infections, but collection from precontinent children is challenging. Each collection method has advantages and limitations. Non-invasive methods (urine pads, bags, clean catch) are convenient but can be time-consuming and are limited by sample contamination. Voiding stimulation methods (bladder-lumbar stimulation, Quick-Wee) can expedite clean catch collection. Invasive methods (catheter, suprapubic aspiration) can be more reliable, but require expertise to perform and cause pain for the child. This article reviews each collection method, and describes collection procedures, indications and strategies to optimise success and reduce contamination.
- general paediatrics
- voiding stimulation
Statistics from Altmetric.com
Introduction
Urinary tract infections (UTI) are one of the most common bacterial infections of early childhood. Among the many febrile young children who present for medical care, approximately 7% will have a UTI.1 Complications of paediatric UTI are uncommon, but can be serious when they occur, including sepsis, meningitis and permanent renal scarring.
UTI in young children cannot be diagnosed reliably without a urine sample. However most young children do not achieve urinary continence until 2–3 years of age in Western society, so collecting urine samples from young children can be challenging.
Who needs a urine sample
Signs and symptoms of UTI in young children are often non-specific. Features such as fever, poor feeding, lethargy and vomiting overlap with many common and benign viral infections, as well as serious bacterial infections. Localising signs such as dysuria (lower UTI: cystitis) or flank pain (upper UTI: pyelonephritis) are uncommon. Clinical diagnosis of UTI in young children is unreliable, so many febrile young children need a urine sample to diagnose or exclude UTI.
Before starting empiric antibiotics for suspected UTI, a urine sample should be collected to confirm the diagnosis.
A urine sample should also be collected from young children with fever without focus, especially if the child is a neonate, younger infant or unwell. Outside early infancy and if the child is not unwell, it may be reasonable to wait 24 hours to see if a focus emerges,2 and if not, then check the urine.
In general, children with a clear alternative focus of illness do not need a urine sample.2 Exceptions include the full septic workup for sick young infants, the child with predisposing features such as renal tract anomalies, the child vulnerable to UTI complications such as solitary kidney and the child with an alternate focus not following the expected course.
What is the urine sample used for
Dipstick and microscopy screening
Urine dipstick testing is a fast and cheap bedside screening tool. Small chemical reagent squares change colour in the presence of specific substrates. Screening for UTI includes checking for nitrites and leucocyte esterase. Urinary nitrites are produced by most but not all uropathogenic bacteria, which convert dietary nitrates into urinary nitrites. Nitrites are highly specific, but not fully sensitive, for UTI. Leucocytes (white blood cells) commonly appear in the urine in response to UTI, but sterile pyuria also occurs with other infections.3 Leucocyte esterase (an enzyme present in leucocytes) is also neither fully sensitive or specific for UTI. Dipstick screening is less reliable in younger infants, as frequent voiding flushes nitrites and leucocytes out of the bladder. While not diagnostic nitrites and leucocytes, particularly when used in combination, are a handy screening tool to indicate if UTI is likely, and to guide initial management.2 3
Urine microscopy can also identify leucocytes and bacteria in the urine, augmenting dipstick screening.
Culture
The gold standard for UTI diagnosis is laboratory urine culture. All major international guidelines recommend culture is used to diagnose UTI in young children.2 4–6 Urine is added to an enriched medium, and considered positive if bacteria grow in sufficient quantity. Results take around 24 hours, at which point the presumptive dipstick diagnosis should be reviewed. Identifying the uropathogen, and its antibiotic sensitivities, guides targeted antibiotic therapy. How much growth on culture is required to diagnose UTI, the colony forming units count, varies between collection methods and local guidelines.4–6 Bacterial growth at lower counts or without pyuria may suggest asymptomatic bacteriuria, contamination or early infection.
Contamination
Contamination is a dirty word when it comes to evaluating UTI. Contamination generally refers to mixed growth of multiple bacterial species. Assuming UTI is caused by a single uropathogen, multiple organisms suggests contamination with incidental skin flora. Contamination corrupts the culture result, as mixed growth may be entirely skin flora, or may conceal a true uropathogen. Incidental skin flora can also lead to false-positive UTI diagnosis if a single species dominates the culture.
Contamination can occur when urine flushes the vagina or glans and foreskin on voiding. Cleaning before collection can reduce the burden of incidental skin flora, although cleaning practices vary. Gauze and sterile water and/or soap may be sufficient for non-invasive collection, but antiseptic cleaning is required before invasive procedures.5
Avoiding contamination is crucial when investigating UTI. For nappy pads and urine bags around half the cultures can be contaminated.7 8 Contamination does not affect dipstick screening, or urine protein and metabolic tests. Differences in how laboratories define contamination (and UTI) can limit comparing contamination rates between different studies and collection methods, although one study has compared contamination between methods at a single centre (table 1).7
Urine sample collection methods for young precontinent children
Invasive versus non-invasive collection
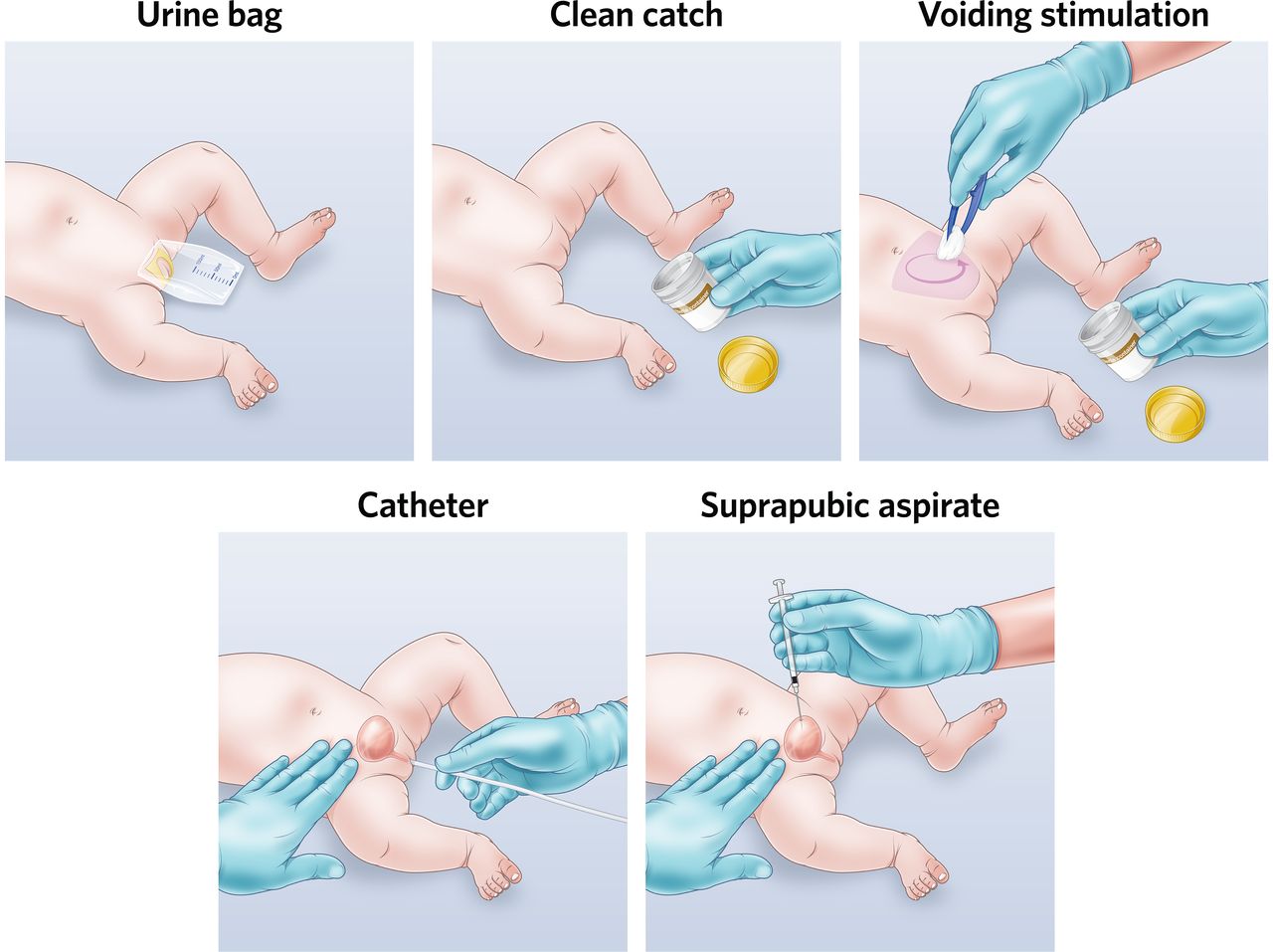
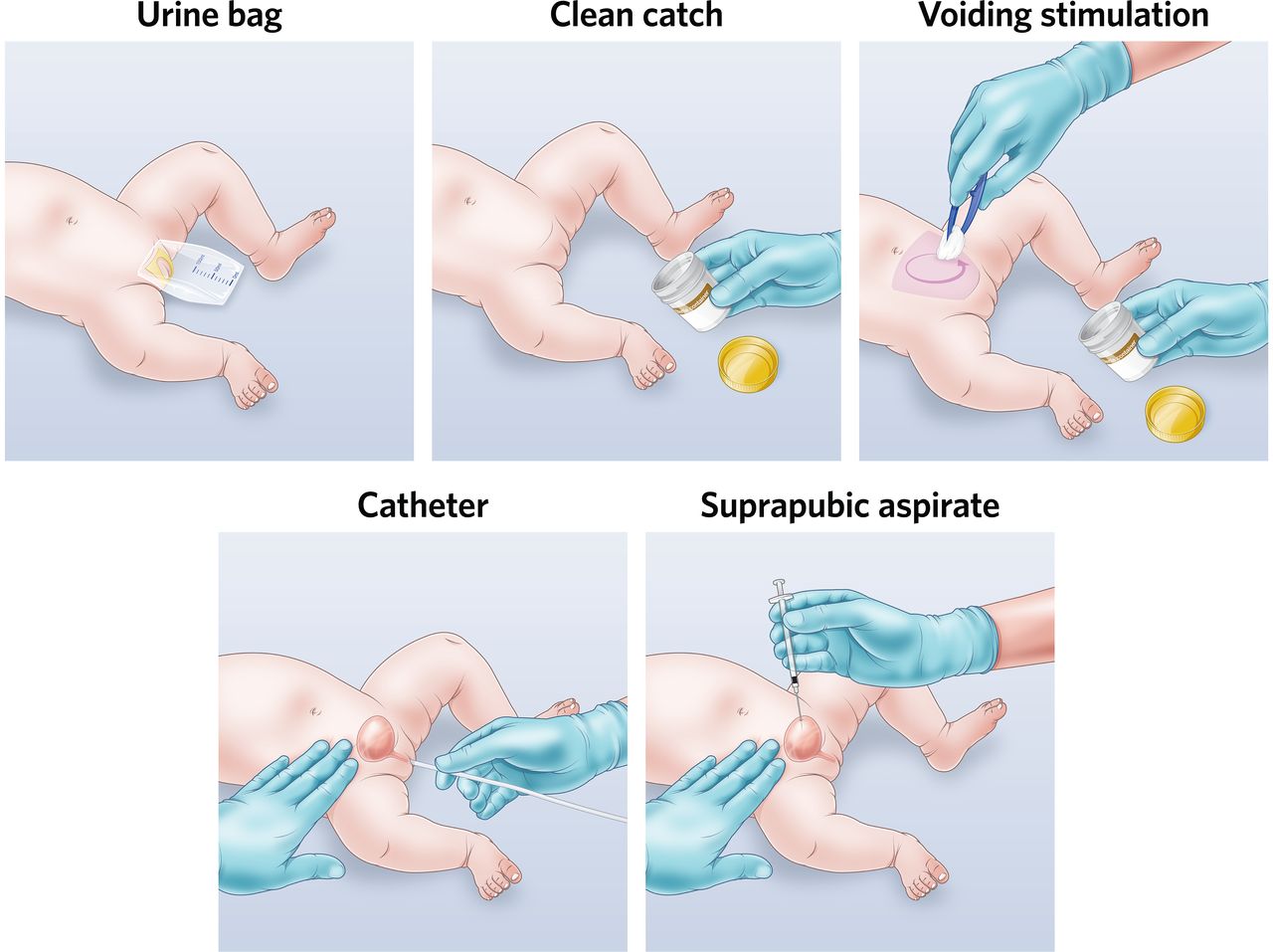
Young children who are not yet toilet-trained cannot void on demand to provide a midstream sample of urine. When facing a febrile precontinent child, other collection methods are required (figure 1).
{kind=link}
Common urine collection methods for young precontinent children. Images by Dr Jonathan Kaufman and Bill Reid, Royal Children’s Hospital.
Non-invasive methods involve waiting for spontaneous voiding, then opportunistically collecting urine in a nappy pad or bag, or ‘clean catch’ of the urine stream. These methods seem convenient and can be done at home by parents, but can be time-consuming, unsuccessful or contaminated. Invasive methods extract urine directly from the bladder by urethral catheterisation or suprapubic needle aspiration (SPA). In skilled hands these methods can be more reliable, but require expertise and equipment to perform, and cause pain and distress to the child.
The optimal collection method remains controversial. All collection methods have advantages and limitations. Accordingly, clinicians and parents have different preferences, and guidelines have different recommendations.2 4
The National Institute for Health and Care Excellence (NICE) UK Guidelines recommend the clean catch method.2 If clean catch is not possible, other non-invasive methods are recommended. Invasive methods are only suggested where non-invasive methods are not possible or practical. In contrast, the American Academy of Pediatrics US Guidelines recommend the opposite, recommending catheter or SPA collection due to lower contamination.4 Non-invasive methods are suggested only for dipstick screening, with invasive collection required to confirm positive screening. Why do these major guidelines have opposing recommendations? Mostly for practical reasons. In the UK, primary care for children is provided by general practitioners who are unlikely to perform invasive collection procedures, while in the USA it is often provided by paediatricians. And elsewhere? Most European guidelines recommend clean catch but acknowledge catheter and SPA as the reference standard, and discourage bag collection except for screening because of contamination (table 2).6 9 10 Australian guidelines recommend clean catch for children who are not too unwell, catheter or SPA for sick infants and discourage sending urine bag for culture.5
International guideline recommendations for urine sample collection for UTI in young precontinent children
Choosing your collection method
Suboptimal sample collection is detrimental to both patient care and health service efficiency. Delayed sample collection increases healthcare resource use. Missed sample collection increases the likelihood of both missed diagnosis and misdiagnosis, which may in turn increase inappropriate antibiotic prescribing and antimicrobial resistance. Optimising sample collection has many benefits.
Choosing the optimal collection method for your patient balances time, equipment, expertise, invasiveness and the likelihood of success and contamination (table 1). In younger and sicker children, an invasive sample is often required to minimise contamination and delay. In older and less unwell children, a clean catch sample may be sufficient. Bag collection is convenient for screening, but false positives and contamination make culture results unreliable. Contamination is a crucial consideration.
Nappy pads and cotton wool balls
Nappy pads are non-invasive and seemingly convenient. Pads are placed inside the nappy, and urine extracted with a syringe after the child voids. However, nappy pads have the highest contamination of all collection methods, reported at over 60% in some settings.11 This is understandable, as they are in close continuous contact with the perineal skin. High contamination makes culture from pad samples highly unreliable.
Cotton wool balls have similar problems with high contamination, and are specifically discouraged by NICE guidance.2
Urine bags
Urine collection bags are another seemingly convenient non-invasive method. The bag is attached over the genitalia with gentle adhesive. They can be placed inside the nappy, or the nappy slit to visualise the bag. They can sometimes leak or detach, and minor discomfort and skin irritation can occur with removal. Average collection time was 85 min in one small observational study,12 and success of bag collection is reported as 82%–96%.12 13
High contamination also makes culture from urine bags unreliable. Like pads, bags are in close contact with the perineal skin. A systematic review including 7659 bag samples from 21 studies found a pooled percentage of 46.6% contamination and 61.1% false positives.8 Many guidelines specifically recommend against sending bag samples for culture due to high contamination.4–6 10 Bag specimens may be helpful for dipstick screening and ruling out UTI, but if positive a more reliable sample should be collected for culture confirmation.4 6
Clean catch
Clean catch is a commonly favoured non-invasive method, and recommended in many guidelines including NICE.2 5 6 Remove the nappy, clean the skin and wait for the child to void spontaneously. Careful attention and quick reflexes are required to catch a sample when they do. The catching task often falls to the parents: a challenge in the middle of the night with a sick child.
Clean catch is not perfectly clean, but has the lowest contamination of non-invasive methods, reported around 10%–25% in most studies.7 11 Take care to minimise contamination. Collectors must avoid touching the inside of the specimen jar, or touching the jar against the child’s skin. While collecting midstream urine is recommended in continent patients to reduce contamination, in precontinent children collecting a definite midstream specimen is difficult.
Clean catch is not always caught, and can be time-consuming. The median time for clean catch attempts in an emergency department (ED) setting is 30 min, with a 64% success rate.14 Most successful clean catches will happen within an hour—after an hour the likelihood of success plateaus significantly.14
So what can be done to expedite clean catch? Offering hydration to increase urine output, and voiding stimulation methods, can increase success.
Voiding stimulation methods for clean catch
Voiding stimulation methods trigger newborn cutaneous voiding reflexes and involuntary urination. Anecdotally, many parents know that changing a nappy often triggers voiding, and many clinicians know that skin cleaning before catheter or SPA procedures can have a similar effect. This suprapubic stimulation triggers reflex parasympathetic bladder contraction. Two voiding stimulation methods have been shown to be effective in clinical trials: the bladder-lumbar stimulation method, and the Quick-Wee method. Most studies evaluate a 5 min stimulation period.
A finger-tap bladder stimulation method to obtain urine samples from babies was first described in 1985, tapping above the pubic symphysis at a rate of one tap per second.15 The subsequently described bladder-lumbar stimulation method uses combined bladder and lumbar stimulation manoeuvres to trigger voiding.16 The baby is held suspended under the armpits with legs dangling, while a second operator applies alternating 30 s stimulation with suprapubic bladder tapping and lumbar circular massage. Success obtaining urine in the neonatal setting is high. In the ED setting, non-randomised trials evaluating a 5 min time period report success of 27% for infants over 1 month of age,17 and 49% for infants 0–6 months of age.18 Maintaining the child’s position can be difficult in older and heavier infants.17
The Quick-Wee method uses cold fluid-soaked gauze to gently rub the suprapubic area in circular motions with the child in the supine position (figure 1) (see online supplementary video).19 The simple single operator method can be performed by doctors, nurses or parents. In a large randomised trial for infants aged 1–12 months, 31% voided within 5 min with Quick-Wee, compared with 12% with standard clean catch, with high parent and clinician satisfaction.
Supplementary file 1
Like other newborn reflexes, cutaneous voiding reflexes diminish with age as volitional bladder control develops, so voiding stimulation methods are more effective in younger infants and in the first year of life.17 18
Catheterisation
Catheterisation involves inserting a catheter (or feeding tube) through the urethra into the bladder, which is removed once urine is obtained, also known as an ‘in-out catheter’ (table 3). Appropriate training and experience is required. Success varies with the operators level of experience, reported between 68% and 100%.20 21
Invasive collection procedures
Contamination with catheterisation is low, at around 10%.7 Discard the first few drops of urine (when possible) to replicate midstream collection and reduce contamination.4 Catheterisation can be successful even with little urine in the bladder, so can be considered after other failed collection attempts.
Catheterisation is invasive and therefore painful. Use age-appropriate procedural analgesia or sedation, although intraurethral anaesthetic gel is no better than non-anaesthetic lubricant for pain reduction.22 The catheter may require some gentle manipulation, but should never be forced. Minor complications such as self-limiting haematuria and dysuria are not uncommon, while serious urethral injury is very rare.
Suprapubic needle aspiration
SPA involves inserting a needle into the bladder through the skin of the lower abdomen, and aspirating urine (table 3). SPA is appropriate for children <2 years of age. Appropriate training and experience is required, although the procedure is quite straightforward once learnt. Success varies with operator experience and volume of urine in the bladder, but is reported as 46%–90%.20 23 Do not remove the nappy until someone with a urine jar is ready for an opportunistic clean catch.
Contamination with SPA is ultra-low, at only 1%.7 Identifying adequate bladder volume with bedside ultrasound before SPA increases success and is recommended,2 although automated bladder scanners are unreliable in infants. Needle insertion does not require ultrasound visualisation. Blind SPA without ultrasound can be performed, but if the child has recently voided, the bladder volume is likely to be low.
SPA is invasive and therefore painful. Use topical anaesthetic cream when possible. Minor haematuria and bruising is relatively common, but serious complications such as needle insertion into the bowel are very rare. Suprapubic abscess, haemoperitoneum and anaerobic bacteraemia have been reported in case reports.
What to do if unsuccessful
Collection attempts are not always successful. Try again, wait, offer fluids to optimise hydration or repeat voiding stimulation. Consider time-limiting non-invasive attempts then trying another method (eg, clean catch is unlikely to be successful after an hour, but catheterisation can be successful even with very little urine in the bladder).
Sometimes collection is unsuccessful despite everyone’s best efforts. Re-evaluate the need for urine collection: has an alternate focus become apparent? The septic infant will require admission, but willing parents can be given provisions to continue clean catch at home for the more well child. Urine samples can be refrigerated once collected, and follow-up arranged if the child remains well.
Conclusion
Collecting urine samples from young children can be challenging. All collection methods have advantages and limitations. Pads and bags have high contamination, so can be used for dipstick screening but culture will be unreliable. Clean catch has the lowest contamination of non-invasive methods and is recommended by NICE guidelines, but can be time-consuming. Clean catch success can be optimised with voiding stimulation methods such as bladder-lumbar stimulation or Quick-Wee. Catheter and SPA can be effective and have lower contamination, but are invasive procedures that require expertise and cause pain for the child. There is no single approach for every patient, clinician or setting, so consider which is best suited, and remember sometimes you just have to go with the flow.
Acknowledgments
The author would like to thank Mr Bill Reid, Royal Children’s Hospital Creative Studio, for his assistance with medical illustrations.
References
Footnotes
Funding JK is supported in part by an Australian Government Research Training Program Scholarship, and Melbourne Children’s Postgraduate Health Research Scholarship.
Competing interests JK is the lead author of previous studies for the Quick-Wee method, which is included in this review.
Provenance and peer review Commissioned; externally peer reviewed.
Republishing keywords: urine specimen collection, infant, urinary tract infection, voiding stimulation, paediatrics
Patient consent for publication Not required.