Article Text

Abstract
Objectives This study examined the effect of using patient-reported outcome measures (PROMs) routinely to assess and address depressive symptoms and diabetes distress among adults with type 2 diabetes.
Design A systematic review of published peer-reviewed studies.
Data sources Medline, Embase, CINAHL Complete, PsycINFO, The Cochrane Library and Cochrane Central Register of Controlled Trials were searched.
Eligibility criteria Studies including adults with type 2 diabetes, published in English, from the inception of the databases to 24 February 2022 inclusive; and where the intervention included completion of a PROM of depressive symptoms and/or diabetes distress, with feedback of the responses to a healthcare professional.
Data extraction and synthesis Using Covidence software, screening and risk of bias assessment were conducted by two reviewers independently with any disagreements resolved by a third reviewer.
Results The search identified 4512 citations, of which 163 full-text citations were assessed for eligibility, and nine studies met the inclusion criteria. Five studies involved assessment of depressive symptoms only, two studies assessed diabetes distress only, and two studies assessed both. All studies had an associated cointervention. When depressive symptoms were assessed (n=7), a statistically significant between-group difference in depressive symptoms was observed in five studies; with a clinically significant (>0.5%) between-group difference in HbA1c in two studies. When diabetes distress was assessed (n=4), one study demonstrated statistically significant difference in depressive symptoms and diabetes distress; with a clinically significant between-group difference in HbA1c observed in two studies.
Conclusion Studies are sparse in which PROMs are used to assess and address depressive symptoms or diabetes distress during routine clinical care of adults with type 2 diabetes. Further research is warranted to understand how to integrate PROMs into clinical care efficiently and determine appropriate interventions to manage identified problem areas.
PROSPERO registration number CRD42020200246.
- %20Type%202">Diabetes Mellitus
- Type 2
- Depression
- Patient Reported Outcome Measures
Data availability statement
Data are available on reasonable request to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The review focuses on depressive symptoms and diabetes distress in people with type 2 diabetes, an important aspect of diabetes management.
Systematic searching of six databases with independent review of abstracts and studies by two reviewers.
Meta-analysis was not possible due to heterogeneity in method and frequency of patient-reported outcome measure (PROM) completion, communication of PROM responses to healthcare professionals and differing associated cointerventions.
Introduction
Type 2 diabetes is a global health priority, with an estimated 463 million people with diabetes in 2017, set to rise to 700 million people in 2045.1 Up to four in ten adults with type 2 diabetes experience emotional health problems, such as depression, anxiety and diabetes distress.2 3 While depression is a general negative affect; diabetes distress is the negative emotional or affective response specific to the day-to-day living with diabetes.3–5 The relationship between diabetes distress and depressive symptoms is bidirectional: elevated diabetes distress is a predictor of future depression, and depression predicts future diabetes distress.6 7 While early studies have linked depressive symptoms to sub-optimal glycaemia8; more recent research has demonstrated that diabetes distress affects glycaemia more than depressive symptoms.5 9 Elevated depressive symptoms and diabetes distress are associated with reduced diabetes self-care and increased risk of diabetes-related complications, impaired quality of life, mortality and an estimated 50% increase in healthcare costs.6 10–15 Recent systematic reviews have focused on interventions for the management of diabetes distress; however, the first step is to identify people with depressive symptoms or diabetes distress requiring interventions in clinical practice.16–18
Guidelines have acknowledged the importance of assessing psychological well-being as part of diabetes care for over 25 years.19 Given the growing evidence that diabetes-tailored psychological interventions reduce elevated distress and glycaemia, international diabetes guidelines have issued recommendations for routine assessment of depressive symptoms and diabetes distress.16 20–25 Guidelines vary in terms of the specific patient-reported outcome measures (PROMs) recommended to assess depressive symptoms or diabetes distress. PROMs are standardised, validated questionnaires to assess latent constructs such as emotional well-being, treatment satisfaction, perceived health or functional status or health-related quality of life.26 Recent consensus from the International Consortium of Health Outcomes Measurement (ICHOM) recommends standardising the assessment of diabetes distress, depressive symptoms and general emotional well-being—with use of the Problem Areas In Diabetes (PAID) scale, Patient Health Questionnaire-9 (PHQ-9) and WHO-Five Well-Being Index (WHO-5), respectively—within clinical diabetes care.27
Despite these recommendations for using PROMs, 60% of healthcare professionals only discuss emotional issues if initiated by the person with diabetes.28 Healthcare professionals need efficient systems to both assess and address depressive symptoms and diabetes distress as part of routine diabetes care.3 For healthcare professionals to use PROMs, they need to understand the utility of PROMs in supporting people with type 2 diabetes clinically, not just for audit or research purposes,29 30 and they need guidance in how to use and interpret PROM responses in clinical consultations.31 32
Thus, the aim of this systematic review is to examine the effect of using PROMs routinely to assess and address depressive symptoms and/or diabetes distress among adults with type 2 diabetes on: (1) glycaemia as measured by HbA1c; (2) self-reported depressive symptoms or diabetes distress; (3) self-reported general emotional well-being or health-related quality of life; (4) self-reported diabetes self-management; (5) referrals for psychiatric or psychological therapy; (6) self-reported quality of patient-professional communication and (7) self-reported satisfaction with the consultation.
Methods
The protocol for this systematic review has been published,33 and the methods are summarised below. We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.34
Eligibility criteria
Inclusion criteria
Studies were eligible if: the design was a randomised controlled trial (RCT), interrupted time-series study, (prospective or retrospective) cohort study, case–control study or analytical cross-sectional study; participants were adults (18 years or older) with type 2 diabetes from any country; interventions involved (1) participants completing a PROM for depressive symptoms and/or diabetes distress and (2) use of PROM responses by the healthcare professional in consultation with the person with type 2 diabetes.
Exclusion criteria
Studies were excluded if they involved: people under 18 years of age, type 1 diabetes or gestational diabetes; or the collection of PROM data but no use of the data in the clinical consultation.
Data sources and searches
A systematic search strategy was used to identify studies. The initial search was on 3 August 2020 and repeated on24 February 2022 using the same search terms (online supplemental file 1). The search was limited to papers published in English and before 24 February 2022. The search strategy was developed in consultation with a librarian from a biomedical library (complete search strategy: online supplemental document 1). Databases searched included MEDLINE (Ovid), EMBASE (Ovid), CINAHL Complete (EBSCO), APA PsycINFO (Ovid), The Cochrane Library (Ovid) and Cochrane Central Register of Controlled Trials (Ovid).
Supplemental material
Study selection and data extraction
Following the initial search on 3 August 2020, two reviewers (RM and a second member of the review team (J-AM-N, BH, LC, DK or FCSH)) screened studies independently based on the inclusion criteria using Covidence software. Both reviewers screened the title and abstract of all eligible studies, followed by full-text screening of the shortlisted studies. Any disagreements about selection, assessment and data extraction in the included studies were discussed between the two reviewers, and if required, a third reviewer was involved in the discussion. Following the updated search on 24 February 2022, RM screened additional identified title and abstract independently, with full-text screening of the shortlisted studies by RM. Reference lists were not checked for studies. Data extraction was undertaken by RM with 20% checked by LC or DK. The extracted data were: study settings, participants, description of the interventions, comparators, study duration, length of follow-up and outcome measures. The authors of the selected studies were contacted for additional data (when published details were insufficient), with 1 month allowed for response.
Quality assessment
Eligible studies were assessed for risk of bias by two reviewers (RM and a second member of the review team (J-AM-N, BH or DK)) independently using the Cochrane Risk of Bias 2 tool or ROBINS-I.35 36 Any disagreements were discussed between the two reviewers, and if required, a third reviewer was involved in the discussion.
Data synthesis
Due to heterogeneity regarding method and frequency of PROM completion, communication of PROM responses to healthcare professionals and differing associated cointerventions (actions based on PROM responses) it was not possible to conduct a meta-analysis. Therefore, the results are summarised narratively.
Patient and public involvement
Patients or public were not involved in the conduct of this systematic review.
Results
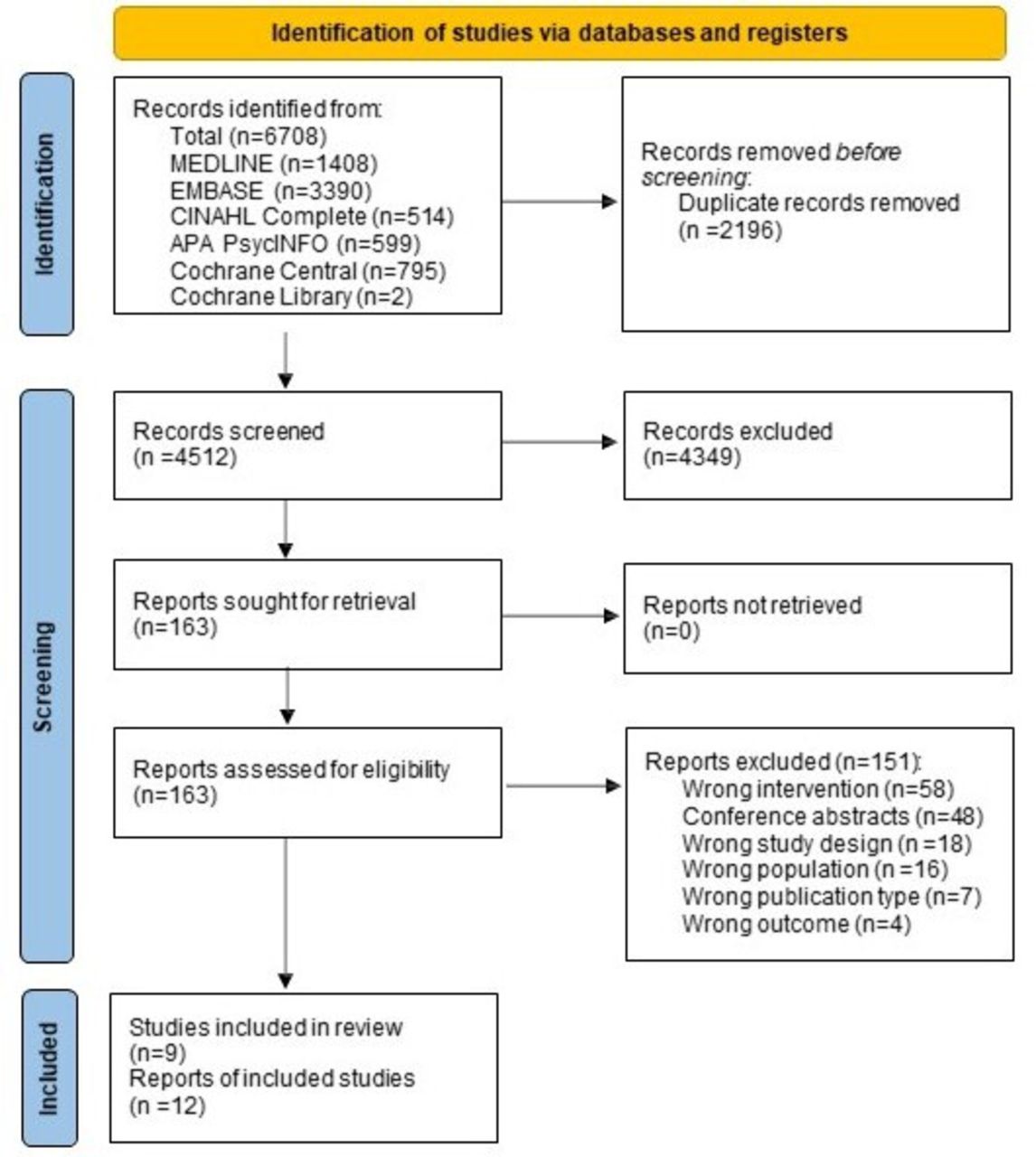
The systematic search identified 4512 citations, of which 163 full-text citations were assessed for eligibility, and 9 studies met the inclusion criteria (figure 1).
{kind=link}
PRISMA flow diagram.34 PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Characteristics of included studies
The nine included studies were published between 2009 and 2020 (table 1). The overall number of participants across all nine studies was N=3325, ranging from N=40 to N=1306 per study. Six of the nine studies were conducted in the USA,37–42 with the remainder conducted in Australia,43 Germany44 and Iceland.45 Most study designs were RCTs (n=6),37 38 one of which was a pilot study (n=1).43 The remaining three studies included case control study (n=2)41 42 and an observational study (n=1).39 Clinical settings varied across studies, including: general practice (n=4)38 40–42; both primary care and hospital clinics (n=2)37 39; specialist outpatient clinic (n=2)43 45 and a specialist rehabilitation service (n=1).44
Study characteristics
Risk of bias of included studies
Four of the nine studies were rated as having a low risk of bias (online supplemental file 2).38 40 41 43 45 Three studies were non-randomised studies of interventions, and at moderate risk of bias due to risk of baseline confounding.39 41 42 Methodological concerns were observed in three studies.37 39 44 Döbler et al reported outcomes for 98 of the 123 participants randomised to the intervention group and did not state how missing outcomes were dealt with; intention to treat was not reported.44 Naik et al reported 12-month outcome data for only 90 of the 136 intervention participants; intention to treat was not reported.37 In most studies, due to the study design, participants and clinical study team members delivering the intervention could not be blinded to participants’ group allocation. Two studies were pilot studies with small sample sizes.43 45 Despite being a pilot study, the Rees et al had sufficient power to detect differences in glycaemia, but lower power for depressive symptoms or diabetes distress.43 Sigurdardottir et al did not include power calculations.45
Supplemental material
Intervention
Interventions to assess depressive symptoms and/or diabetes distress
Five of the nine studies assessed depressive symptoms alone,37–39 41 42 two assessed depressive symptoms and diabetes distress,40 44 and two assessed diabetes distress alone.43 45 All seven studies assessing depressive symptoms used the PHQ.37–42 44 One study used the PHQ-2 for brief screening with responses of more than three proceeding to the PHQ-9.39 Diabetes distress was assessed in two studies using the Diabetes Distress Scale (DDS)40 43 and in two studies using the PAID scale.44 45
PROMs were completed either in-person (n=5),40–44 or via telephone (n=4).37–39 45 In six studies, PROM responses were collected by study team members not involved in ongoing clinical care,37 38 40 41 43 44 either via telephone,37 38 41 44 or at the clinic with a study team member.40 43 One study collected PROM responses using automated calls.39 In two study, PROM completion was at the clinic with the diabetes educator.42 45
Feedback of PROM responses provided to treating healthcare professionals varied. Three studies trained case managers in making treatment recommendations to primary care health professionals based on case collaboration and treatment algorithms.38 41 42 In studies where trained study members collected PROM responses, the mechanism by which PROM data were provided to the treating healthcare professionals was not reported.43 44 In the Naik et al study, the general practitioner received a secure message notifying the HbA1c results and PHQ-9 response.37 Wu et al used PHQ-9 responses to generate action reminders integrated with the disease management registry for healthcare professionals to review.39
Cointervention associated with PROM responses
Each of the nine studies had a cointervention associated with the PROM completion (see table 1), which included telephone-assisted psychological therapy or coaching interventions,37 40 43–45 or healthcare professional interventions of collaborative team care with case management and stepped care treatment algorithms.38 41 42 Wu et al linked PROM responses to a clinical decision support tool that generated action reminders for healthcare professionals based on PROM responses within a disease management register.39
Outcomes
Reported outcomes across studies are detailed in table 2. Referrals to psychology or psychiatry services were not reported. In three studies, in the control arm, healthcare professionals were informed of the elevated depressive symptoms.37 38 41 In no study were healthcare professionals informed about elevated diabetes distress of participants in the control group.
Follow-up study outcomes between intervention and control groups
All nine studies reported glycaemia, measured by HbA1c, as an outcome measure. Where PROM assessed depressive symptoms (n=7), a clinically significant between-group difference in HbA1c was observed in two studies.42 44 Where diabetes distress was assessed (n=4), a clinically significant between-group difference in HbA1c was observed in two studies.43 44 Each of these studies had a cointervention involving a series of psychological therapy sessions.43 44 Only one of three studies using PROMs as part of stepped care algorithms with care coordination demonstrated a statistically significant glycaemic reduction.42
All but two studies examined the impact of PROMs use on depressive symptoms.42 45 Across all seven studies, depressive symptoms (measured with the PHQ-9) reduced in both arms. Where the intervention included assessment of depressive symptoms (n=7), statistically significant difference in depressive symptoms between groups was observed in five studies.37–41 Where diabetes distress was assessed during the intervention (n=4),40 43–45 three studies40 43 44 reported depressive symptoms as an outcome measure, with a significant difference in depressive symptoms between groups observed in one study.40 Five studies reported diabetes distress as an outcome measure.40 41 43–45 Diabetes distress reduced in both the intervention and control arms across all five studies.40 41 43–45 The difference between groups, favouring the intervention, was statistically significant in two studies.40 41
In the Cummings et al study, when therapy was stratified based on elevated levels of depressive symptoms or diabetes distress, improved diabetes self-management was reported.40 Similarly, in the Rees et al study, when cointerventions focused on people with type 2 diabetes with elevated distress levels receiving individual psychological therapy, an improvement in diabetes self-management was reported.43 General emotional well-being, mental health and health status were reported using various measures, including the WHO-5, Well-being Questionnaire (W-BQ), 12-Item Short-Form Survey and EQ-5D. No study reported patient–professional communication as an outcome. The Wu et al study was the only one to assess satisfaction with diabetes care, and a statistically significant improvement in the intervention arm was observed.39
Discussion
Main findings
To our knowledge, this is the first systematic review to synthesise the evidence related to PROM use to assess and address depressive symptoms and/or diabetes distress in type 2 diabetes care, despite diabetes guidelines recommending this practice for the past 25 years.20–25 The key finding is that very few studies have examined the use of PROMs to assess and address depressive symptoms and/or diabetes distress during routine type 2 diabetes care. When depressive symptoms were assessed (n=7), a statistically significant between-group difference in HbA1c was observed in two studies.42 44 A statistically significant between-group difference in depressive symptoms was observed in five of six studies where depressive symptoms were assessed during the intervention.37–41 Where diabetes distress was assessed, a clinically significant between-group difference in HbA1c (glycated hemoglobin) was observed in two of four studies,43 44 and a statistically significant difference in both depressive symptoms and diabetes distress was observed in one study.40 Two studies targeting people with elevated diabetes distress or depressive symptoms demonstrated statistically and clinically significant reductions in glycaemia.43 44 This review found little evidence of the best-associated cointervention for people identified by PROMs with elevated depressive symptoms or diabetes distress despite guideline recommendations.20–25
Similar to this review’s findings, a Cochrane review of PROM completion and feedback to healthcare professionals in the treatment of mental health conditions found insufficient evidence of impact on patient outcomes.46 However, the interventions included in the Cochrane review were limited to PROM feedback to the healthcare professional, not linked to interventions.46 While healthcare professionals frequently treat coexisting depression and type 2 diabetes, emotional issues such as diabetes distress are discussed less frequently.28 While over 238 unique PROMs for people with type 2 diabetes have been identified, the most effective intervention to implement and then address PROM-identified elevated depressive symptoms or diabetes distress remains unclear.47 Details about how precisely PROMs were used by healthcare professionals in discussion with people with type 2 diabetes were lacking. Further exploration of how PROMs can be integrated into routine clinical practice with the escalation of care for people with elevated depressive symptoms or distress is needed. Considering the recent recommendations from ICHOM for PROM use during diabetes care,27 healthcare professionals need guidance on the appropriate evidence-based intervention for elevated depressive symptoms or diabetes distress identified using a PROM in clinical practice.29 30
Studies demonstrating improved glycaemia had cointerventions of targeting people with elevated distress levels or depressive symptoms.43 44 Döbler et al increased frequency of follow-up counselling if elevated depressive symptoms were identified using the PHQ-9.44 Sturt’s systematic review regarding the effectiveness of interventions to reduce diabetes distress showed that interventions delivered by a general healthcare professional demonstrate an improvement in glycaemia and reduce diabetes distress.17 However, participants included in Sturt’s review had low levels of diabetes distress, and a further systematic review in 2018 identified that severe diabetes distress reduced with diabetes-specific psychological interventions.16 Evidentially, targeted interventions are needed stratified on the basis of severity of distress.
Studies have reported that completing a measure of diabetes distress before a consultation can improve glycaemia and patient satisfaction among adults with type 1 and type 2 diabetes.48 However, only Wu et al 39 explored changes in patient satisfaction with care—which is an important measure considering PROMs are reported as enablers of person-centred care.39 49 No studies in our review explored the impact on patient-professional communication in the consultation, despite evidence suggesting PROM use in other clinical settings (oncology) improves communication, with PROMs initiating discussion of issues not otherwise addressed.50
Studies have also indicated that completion of a diabetes distress measure before a consultation, and discussion of those responses during the consultation, improves glycaemia and reduces diabetes distress among adults with type 1 and type 2 diabetes in specialist diabetes clinics.7 48 Pouwer et al’s study of people with type 1 and type 2 diabetes found monitoring of well-being, using the W-BQ, during diabetes care resulted in improved mood.51 While PROMs in these studies were embedded in routine care, they included people with type 1 and type 2 diabetes (without separate sub-group analyses) and were not conducted in general practice, where most type 2 diabetes care occurs.52 In our review, PROMs were completed most frequently with a trained study team member, not by a healthcare professional involved in the person’s clinical care.37 38 40 41 43 44 While this may replicate the likely real-world administration of PROMs (eg, by a receptionist, on arrival at the clinic), it is suggested that screening for depressive symptoms is best performed as part of collaborative care by the treating doctor or diabetes educator.53 In the future, it would be useful to explore models based on depressive symptoms or diabetes distress identified by the usual healthcare professional with stratification of actions based on responses.
Healthcare professionals need PROMs that provide responses that provoke action. However, the effective interventions in this study were resource-intensive, which will be difficult to replicate and sustain in routine clinical practice. Only one study used electronic prompts to healthcare professionals based on PHQ responses.39 Several studies have highlighted that clinical systems for PROM response delivery to healthcare professionals need to fit with clinical workflow.54–56 Even with the electronic delivery of PROM responses, the large volume of responses for healthcare professionals to review and the difficulty accessing PROM responses (due to storage on a dashboard separate from the electronic medical record) contribute to low use of PROMs in clinical settings.55–57
Strengths and limitations of the review
Key strengths of this review include adherence to the PRISMA guidelines,34 a comprehensive search strategy of six electronic databases and screening performed independently by two reviewers. The risk of bias was low in most studies, indicating outcomes of this review are based on high-quality studies. Depression and diabetes distress were assessed using well-validated measures, including PHQ, PAID and the DDS. The focus on type 2 diabetes is also a strength, as people with type 2 diabetes receive their care mostly in primary care settings, and their needs and preferences are different from people with type 1 diabetes.58 59
The heterogeneity of included cointerventions, how PROMs were completed, and healthcare professionals received the PROM responses, limits the overall review, making comparisons between studies difficult. It was not possible to conduct a meta-analysis because of the wide range of interventions and cointerventions assessed. Two studies had a small sample size with limited statistical power.43 45 Other limitations include the restriction of our search to published journal articles in the English language. This may explain why all studies included were from high-income or upper-middle-income countries, with no studies from low-middle-income countries identified. The inclusion criteria limited studies to populations with type 2 diabetes only, or where a subgroup analysis of participants with type 2 diabetes was included.
Future directions
Considering the low number of eligible studies, further research is warranted to understand the most efficient cointerventions to associate with PROM responses and how to integrate PROMs to coordinate interventions in general practice where most type 2 diabetes care occurs. The interventions examined as part of this review required significant external staff involvement, while only one study used technology to assist with PROM collection and delivery to healthcare professionals. Future research could focus on similar interventions using technology for self-completing PROMs with actionable outcomes if elevated depressive symptoms or diabetes distress are identified. Further research is needed to explore if PROM assessment of depressive symptoms and diabetes distress in routine type 2 diabetes care impacts communication and patient satisfaction with care.
Conclusions
This systematic review summarised and critiqued studies using PROMs for assessing and addressing depressive symptoms and/or diabetes distress as part of clinical type 2 diabetes care. The findings showed few studies using PROMs, but most are effective in reducing depressive symptoms or diabetes distress, though cointerventions related to PROM use in type 2 diabetes care are heterogeneous. While guidelines recommend the routine assessment of depressive symptoms and diabetes distress using PROMs, a clear mechanism for implementing this in routine diabetes care or the most effective cointervention is yet to be established.
Data availability statement
Data are available on reasonable request to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This is a systematic review, ethical approval was not required.
Acknowledgments
The authors acknowledge the support of the University of Melbourne librarians Wil Villareal and Patrick Condon with preparing the search strategy
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @janespeight, @jo_manski
Contributors RM, J-AM-N, BH, JE, JS and CH conceived the study. RM, J-AM-N, BH, DK, LC and FCSH performed the citation screening and risk of bias assessments. RM extracted the data with 20% also extracted by LC. RM drafted the manuscript and revised it based on the feedback from coauthors. RM is the acting guarantor and accepts full responsibility for the work/manuscript, she has access to data, controlled the decision to publish. All authors approved the manuscript for submission.
Funding RM receives a PhD scholarship from Australian Rotary Health and the University of Melbourne (Grant number is not applicable). CH and JS are supported by core funding to the Australian Centre for Behavioural Research in Diabetes provided by the collaboration between Diabetes Victoria and Deakin University.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.