Article Text

Abstract
Objectives Timely recognition and treatment of sepsis is essential to reduce mortality and morbidity. Acutely ill patients often consult a general practitioner (GP) as the first healthcare provider. During out-of-hours, GP cooperatives deliver this care in the Netherlands. The aim of this study is to explore the role of these GP cooperatives in the care for patients with sepsis.
Design Retrospective study of patient records from both the hospital and the GP cooperative.
Setting An intensive care unit (ICU) of a general hospital in the Netherlands, and the colocated GP cooperative serving 260 000 inhabitants.
Participants We used data from 263 patients who were admitted to the ICU due to community-acquired sepsis between January 2011 and December 2015.
Main outcome measures Contact with the GP cooperative within 72 hours prior to hospital admission, type of contact, delay from the contact until hospital arrival, GP diagnosis, initial vital signs and laboratory values, and hospital mortality.
Results Of 263 patients admitted to the ICU, 127 (48.3%) had prior GP cooperative contacts. These contacts concerned home visits (59.1%), clinic consultations (18.1%), direct ambulance deployment (12.6%) or telephone advice (10.2%). Patients assessed by a GP were referred in 64% after the first contact. The median delay to hospital arrival was 1.7 hours. The GP had not suspected an infection in 43% of the patients. In this group, the in-hospital mortality rate was significantly higher compared with patients with suspected infections (41.9% vs 17.6%). Mortality difference remained significant after correction for confounders.
Conclusion GP cooperatives play an important role in prehospital management of sepsis and recognition of sepsis in this setting proved difficult. Efforts to improve management of sepsis in out-of-hours primary care should not be limited to patients with a suspected infection, but also include severely ill patients without clear signs of infection.
- sepsis
- diagnosis
- after hours care
- primary care
- general practice
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study into the management of sepsis in out-of-hours primary care.
Combining information from the electronic medical records of the hospital and general practitioner cooperative resulted in complete data.
As only patients with sepsis admitted to the intensive care unit were included in the study, data from other patients with sepsis are lacking.
The retrospective nature of the study does not allow us to draw causal relations between the management in primary care and outcome.
Introduction
Sepsis is a life-threatening complication from infection requiring urgent hospital treatment.1 2 One in four patients with sepsis die during hospitalisation, and sepsis survivors often suffer from long-term functional and cognitive impairment.2 3 Sepsis is one of the most common reasons for intensive care unit (ICU) admission, and is associated with high healthcare costs.4 Estimations of the incidence of community-acquired sepsis range between 40 and 455 per 100 000.5 Over the last decades epidemiological data show a rising incidence of sepsis.6 7 Due to the ageing population, a further increase of the sepsis incidence is expected.8
In 2004, the Surviving Sepsis Campaign (SSC) was launched internationally.9 Mainly owing to the implementation of screening tools for early recognition of sepsis in the emergency department (ED), the SSC succeeded to reduce in-hospital mortality by 17% in the Netherlands.10 Research in patients transported by ambulance shows that recognition of sepsis in the prehospital setting is low.11 12 Most patients with sepsis initially contact a general practitioner (GP), and the assessment by the GP, including the decision whether or not to refer a patient to secondary care, is crucial for timely initiation of hospital treatment. Recording of vital signs is essential, but, compared with secondary care doctors, GPs generally use more factors such as clinical impression and gut feeling in their diagnostic work-up.13 However, rigorous data on diagnostic accuracy and appropriateness of sepsis management in primary care are not available.
In the Netherlands, out-of-hours primary care is delivered by large scale GP cooperatives that are in about 65% colocated with hospital ED.14 A total of 120 GP cooperatives provide out-of-hours primary care for all inhabitants of the Netherlands.15 As sepsis typically presents as an acute illness in which assessment cannot wait until the next day, we expect a large proportion of all patients with sepsis contacting a GP cooperative prior to hospital admission.The aim of this study is to investigate the diagnosis and management at the out-of-hours GP cooperative of patients who were subsequently admitted to ICU for community-acquired sepsis. This information is needed to better target interventions and further research to improve the management of sepsis in primary care.
Methods
Design and setting
A retrospective study of medical records of patients admitted to the ICU of Gelderse Vallei Hospital, Ede, the Netherlands, for community-onset sepsis was conducted. Data were retrieved from patients admitted between 1 January 2011 and 31 December 2015. Gelderse Vallei Hospital is a general hospital with 605 hospital beds and a 17 beds level 3 ICU, to serve a mainly suburban population of 260 000 inhabitants. Over 22 000 patients visit the ED annually. A large GP cooperative for out-of-hours primary care is colocated adjacent to the hospitals’ ED and serves a similar catchment area as the hospital. Patients contact the GP cooperative by telephone. Subsequently, a triage nurse supervised by a GP decides whether a telephone advice, clinic consultation, home visit or immediate ambulance deployment is needed, and with which urgency.
Patients
Patients were selected using the following inclusion criteria: age ≥18 years; admitted to the ICU within 24 hours from hospital arrival; sepsis diagnosis during ICU stay. In the hospital, all patients admitted to the ICU are screened with an electronic tool to assess the presence of sepsis. These data are recorded in the patient data management system (PDMS). The presence of sepsis in this registration system is based on the ACCP/SCCM sepsis consensus definitions.16
The medical records of the included patients were subsequently screened (by FJL and ARHvZ) for the following exclusion criteria: sepsis not the primary reason for ICU admission; readmissions after hospitalisation <7 days earlier; patients referred to the ED by the GP cooperative, but not admitted after initial ED assessment (as delay to hospital treatment is not caused by the GP in these patients); medical treatment with close secondary care follow-up (eg, chemotherapy with possible neutropenia, as typically these patients bypass the GP by consulting secondary care directly); transfer from or to another hospital; home address outside the catchment area of the GP cooperative at the time of admission.
Data collection
We digitally collected the following routine registration data from the electronic medical records of the ICU: age, sex, Sepsis-related Organ Failure Assessment (SOFA) score, Acute Physiology and Chronic Health Evaluation (APACHE) II score, immunosuppressive status, length of ICU stay, length of hospital stay and in-hospital mortality. Additional data from the electronic hospital records were retrieved by manual search (by FJL): comorbidities, vital signs (tympanic temperature, systolic blood pressure, heart rate, respiratory rate and mental status), laboratory values (C reactive protein (CRP), lactate and creatinine), presence of septic shock and final diagnosis. For both vital signs and laboratory values, the first recorded values in the first 24 hours after ED arrival were used. If a parameter was not recorded in the first 24 hours after ED arrival, this was entered as missing data. Mental status was considered as altered in case of a Glasgow Coma Scale <15 or an otherwise recorded altered mental status in the medical records. The final diagnosis regarding the presence of sepsis and site of infection was based on the review of all available medical records. In case of equivocal diagnosis in the medical records, a consulted intensivist made the final decision.
Septic shock was defined as the prolonged use of vasopressors to maintain a mean arterial pressure of ≥65 mm Hg after fluid resuscitation. The comorbidities were recorded as documented in the discharge letter of the ED. Cardiovascular disease was present in case coronary artery disease, heart failure or stroke was noted. Malignancy was reported in case any malignancy was noted, except for basalioma or if curative treatment had taken place >5 years ago. Multimorbidity was defined as the presence of two or more recorded comorbidities.
Subsequently, we retrieved data from the included patients from the electronic medical records of the GP cooperative. All contacts from the last 72 hours before hospital admission were analysed. The time of the first telephone contact was recorded, as well as the urgency category after telephone triage, type of consultation, clinical signs, diagnosis and referral. Suspected infection was defined as the diagnosis of an infectious disease or mentioning of an infectious cause in one of the first three differential diagnoses in the free text.
Statistical analysis
Analyses were performed using IBM SPSS V.22. Descriptive analyses were used for frequencies, time intervals and outcome. For normal distributions means and SD were used, while median and IQRs were used in case of skewed distributions. For comparison of continuous variables, Student’s t-tests were used for normal distributions and Mann-Whitney U tests for skewed distributions. Pearson’s χ2 test was used for nominal variables. After univariate regression analyses, all variables with a p<0.1 were subsequently tested in a multivariable logistic regression model to explore associations with mortality. Results were considered significant at p<0.05.
Patient involvement
No patients were involved in setting the research question or the outcome measures, nor were they involved in developing plans for design or implementation of the study. No patients were asked to advise on interpretation or writing up of results. The results of this study are used for the planning of further research in which patients are involved and of which the results will be disseminated in the relevant patient community.
Results
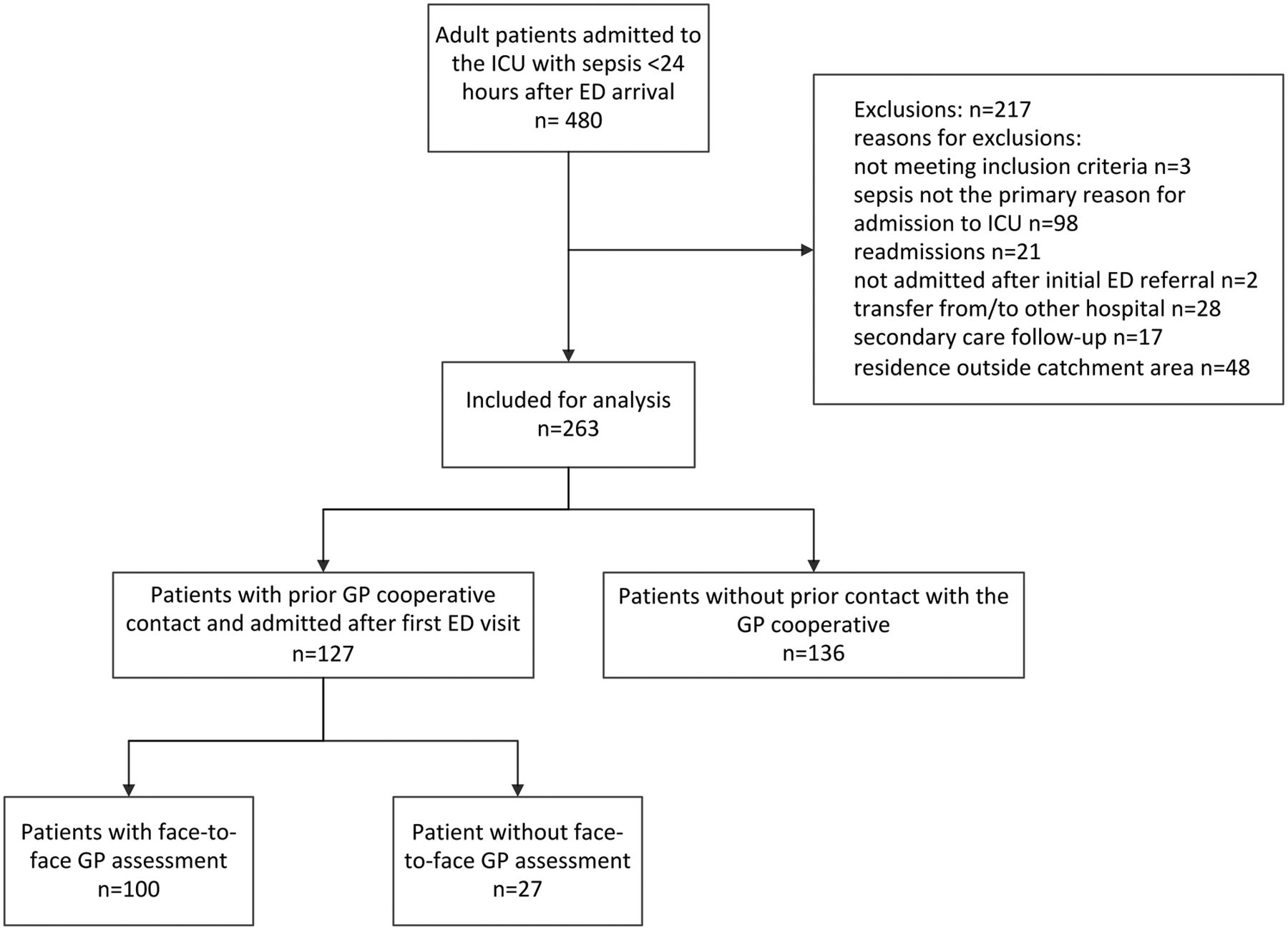
A total of 480 patients with sepsis were identified using an automated search of the PDMS. After reviewing the medical records, 217 patients were excluded (figure 1). Of the included 263 patients, 127 patients (48.2%) had previous contact(s) with the GP cooperative in the 72 hours before hospital admission. In total, 97/127 patients (76.4%) had one contact with the GP cooperative prior to the hospital admission, 23/127 (18.1%) had two contacts and 7/127 (5.5%) more than two. There were no statistically significant differences between the characteristics of the patients with and without prior GP cooperative contact (table 1). Of all included patients, 140/263 (53.2%) arrived at the ED during out-of-hours. Of the patients arriving out-of-hours at the ED, 75.7% had contacted the GP cooperative in the previous 72 hours, compared with 17.1% of the patients arriving in hours (data not shown in table).
Patient characteristics and outcomes of patients with sepsis with and without prior GP cooperative contact
{kind=link}
Flow chart of study population. ED, emergency department; GP, general practitioner; ICU, intensive care unit.
The 127 patients who had prior contact with the GP cooperative were further analysed (table 2). In 16 cases (12.6%), the patient was directly transferred to the hospital by an ambulance, after telephone triage and without face-to-face GP assessment. In 76 cases (59.8%), a home visit followed after telephone triage, and in 24 cases (18.9%) a face-to-face consultation at the GP cooperative was performed (clinic consultation). The remaining 11 cases (8.7%) received telephone advice. Sixty-three per cent of the patients received a highly urgent triage category (U1 or U2) after telephone triage. In patients assessed during a home visit, 50/76 (65.8%) were referred to the hospital after this initial contact, compared with 14/24 (58.3%) of the patients receiving a clinic consultation. The median delay to hospital arrival was 1.7 hours for the total cohort. As expected, the median delay in case of immediate ambulance deployment was shorter (median 1.0 hour), and longer after only telephone advice (median 15.1 hours). Mortality rates in the different subgroups had a wide range (0.0%–38.1%), but the subgroups were too small to reach statistically significant differences.
Hospital referral, prehospital time delay and hospital mortality of patients with sepsis who had contacted the GP cooperative (n=127), according to type of contact and triage urgency category after telephone triage†
One hundred patients (76 home visits and 24 clinic consultations) received a face-to-face assessment by a GP (table 3). In 57/100 cases, an infection was either diagnosed or suspected, and in only six cases this was documented as sepsis or possible sepsis (not shown in table). In case that infection was not suspected after the initial GP assessment, the mortality rate was higher compared with patients with suspected infection (41.9% vs 15.8%). The patients without suspicion of infection were older (mean age 71 years, vs 65 years). In this group, respiratory rate and temperature were less frequently recorded, as well as the total number of vital signs (1.6 compared with 2.4). Fever (temperature >38˚C) was recorded more frequently when infection was suspected (54.4% compared with 11.6% in patients without suspected infection). There was no association between delay and hospital mortality. In the multivariable logistic regression model (table 4), the increased mortality when infection was not suspected remained statistically significant after corrections for the possible confounders age, multimorbidity, APACHE II score and SOFA score.
Characteristics and clinical findings of patients with sepsis who had face-to-face GP assessment (n=100), in whom infection was suspected or not suspected
Multivariable logistic regression model for in-hospital mortality of patients with sepsis who received face-to-face GP assessment (n=100)*
In patients who were referred to the ED after the first GP assessment, the mortality rate of patients in whom infection was suspected was 12.5%, compared with 56.0% when the GP did not suspect infection. In patients not referred after the first contact, hospital mortality was 22.2% in both groups (data not show in table).
Discussion
We found that 48% of the patients admitted to the ICU for community-acquired sepsis had contacted the GP cooperative for out-of-hours primary care prior to admission. The most important new finding is that in 43% of these patients the GP did not suspect an infection, and mortality rates were almost three times higher in this group compared with patients with sepsis in whom the GP suspected infection during the initial contact.
The patients with sepsis in whom infection was not suspected by the GP were on average 5 years older. This may indicate that infections are more difficult to identify in the elderly. As sepsis-related mortality increases with age, this can partially explain the difference in mortality between the two groups, but the difference remained statistically significant after adjustment for age and other possible confounders. The failure to suspect infection in a patients with sepsis might delay adequate treatment, even if the GP decides to refer the patient. For example, several patients in our cohort were referred to a cardiologist with suspicion of acute decompensated heart failure and initially treated with furosemide. Roest et al found similar results in a retrospective cohort of patient with sepsis transported to hospital by ambulance.12 In 42% of the transported patients, sepsis was not documented and mortality was significantly higher in this group (26% in non-documented sepsis vs 13% in patients with documented sepsis).
However, patients without clear signs of infection might also have a worse prognosis regardless the treatment. In a large retrospective study in patients with community-acquired sepsis admitted to 1 of 30 ICUs in Sweden, an inverse correlation was found between body temperature at presentation in the ED, and mortality.17 Not only hypothermic, but also normothermic patients showed higher mortality compared with febrile patients who could not be attributed to other risk factors or treatment. We cannot predict the effect on mortality should the GP recognise sepsis in all patients correctly, but the subgroup of patients in whom infection was not suspected seems to be the most severely ill group of patients which cannot be ignored in efforts to decrease sepsis-related mortality.
In our study, approximately two-thirds of the patients were referred after the initial GP consultation. Other studies investigating the management of sepsis in general practice were not found, though the recognition and management of meningococcal disease in children by GPs has been reported.18 In about half of these cases the GP referred the patient to the hospital after the first assessment, which is slightly lower than in our study. These findings suggest that serious infections can be difficult to recognise in general practice, even within hours before the infection is imminent life threatening.
Implications for practice and further research
The out-of-hours home visit should be considered as a high-risk setting for the prevalence of sepsis, as one in three patients admitted to the ICU with sepsis was assessed during a home visit of the GP cooperative prior to the hospital admission. Patients with sepsis are therefore heavily over-represented in this setting, as out-of-hours home visits only account for around 0.5% of all GP contacts and 10% of GP cooperative contacts.14 As early initiation of adequate treatment of sepsis is crucial to improve outcome, prehospital delay should be minimised. Ideally, every patient needing ICU treatment for sepsis should be directly transported by ambulance to the ED. The lack of association between delay and mortality in this study does not imply delay is irrelevant for the outcome. More severely ill patients are generally transported to the hospital more quickly. Therefore, it was expected that patients with short delay presented high mortality rates. The finding that the most severely ill patients, who were directly transported to the ED by ambulance presented relatively low mortality rates (19%), suggest immediate ambulance deployment is beneficial for these patients.
On the other hand, unnecessary referrals should be prevented. Therefore, quick assessment by a GP is warranted in case the need for hospital treatment is equivocal after telephone triage. Comprehensive measurements of relevant vital signs might facilitate detection of sepsis. As in almost half of the patients infection was not suspected, sepsis should also be considered in patients who are acutely ill without obvious signs of infection, especially among elderly patients. As only 30% of the patients presented with fever, point-of-care (POC) testing can possibly identify infection better than physical examination alone. CRP values were strongly elevated in most patients who were not considered as having an infection. POC-CRP testing is increasingly available in primary care, and it is feasible to implement this during home visits. However, not all patients with sepsis have (strongly) elevated CRP levels, and not all patients with elevated CRP levels need hospital treatment. Procalcitonin is possibly superior to CRP for the diagnosis of sepsis and should also be investigated, as also recommended in the National Institute for Health and Care Excellence guidelines for the diagnosis and management of sepsis published in 2016.19 Prospective research in the primary care setting is needed to investigate the diagnostic and prognostic value of both clinical findings as well as biomarkers available as rapid bedside tests.
Strengths and limitations
The major strength of the study is the linking of data from the electronic medical records from the ICU and the GP cooperative, resulting in complete data for the main outcome measures of all included patients. Manual retrieval of additional data from the hospital medical records provided more contextual information. However, several limitations have to be mentioned. The study was performed in one large general hospital. Results may not be the same for other areas in the Netherlands or other countries. Another limitation of the study is the retrospective design and selection of patients requiring ICU treatment for sepsis. Patients with sepsis who were promptly recognised and urgently referred to the ED by a GP may have been treated successfully in regular wards, and therefore did not receive ICU treatment. This may have resulted in a selection of patients who were treated less adequately in the prehospital phase. However, this would then also imply that ICU admissions could be prevented if detection by the GP is improved.
Conclusions
GPs’ clinical detection of sepsis in primary care proves to be difficult. More than one-third of ICU admitted patients with sepsis initially assessed by GPs in out-of-hours primary care were not referred to a hospital. In almost half of the patients the GP had not suspected an infection. The highest mortality rates were observed in those patients in whom GPs had not suspected an infection. Efforts to improve identification and management of sepsis in the primary care setting should not be limited to patients with obvious signs of infection, but also include acutely ill patients without a clear diagnosis.
Acknowledgments
The authors would like to thank Dick van Blokland for the digital extraction of patient data from the PDMS of the ICU, other employees of Gelderse Vallei Hospital involved and all involved collaborators of the colocated GP cooperative (Huisartsenpost Gelderse Vallei) for their cooperation in this study.
References
Footnotes
Contributors FJL and PG conceived the study. MS and ARHvZ helped in its design. FJL, MS, CvS and ARHvZ were responsible for data assembly, collection and analysis. FJL, RMH and ARHvZ were responsible for data interpretation. FJL drafted the manuscript. MS, RMH, PG and ARHvZ provided significant revisions for important intellectual content. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval The medical ethics committee of the Radboud university medical center Nijmegen approved the study (file number 2015-2209).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.