Article Text

Abstract
Objective To establish the level of opioid prescribing for patients with chronic musculoskeletal pain in a sample of patients from primary care and to estimate prescription costs.
Design Secondary data analyses from a two-arm pragmatic randomised controlled trial (COPERS) testing the effectiveness of group self-management course and usual care against relaxation and usual care for patients with chronic musculoskeletal pain (ISRCTN 24426731).
Setting 25 general practices and two community musculoskeletal services in the UK (London and Midlands).
Participants 703 chronic pain participants; 81% white, 67% female, enrolled in the COPERS trial.
Main outcome measures Anonymised prescribing data over 12 months extracted from GP electronic records.
Results Of the 703 trial participants with chronic musculoskeletal pain, 413 (59%) patients were prescribed opioids. Among those prescribed an opioid, the number of opioid prescriptions varied from 1 to 52 per year. A total of 3319 opioid prescriptions were issued over the study period, of which 53% (1768/3319) were for strong opioids (tramadol, buprenorphine, morphine, oxycodone, fentanyl and tapentadol). The mean number of opioid prescriptions per patient prescribed any opioid was 8.0 (SD=7.9). A third of patients on opioids were prescribed more than one type of opioid; the most frequent combinations were: codeine plus tramadol and codeine plus morphine. The cost of opioid prescriptions per patient per year varied from £3 to £4844. The average annual prescription cost was £24 (SD=29) for patients prescribed weak opioids and £174 (SD=421) for patients prescribed strong opioids. Approximately 40% of patients received >3 prescriptions of strong opioids per year, with an annual cost of £236 per person.
Conclusions Long-term prescribing of opioids for chronic musculoskeletal pain is common in primary care. For over a quarter of patients receiving strong opioids, these drugs may have been overprescribed according to national guidelines.
Trial registration number ISRCTN24426731; Post-results.
- opioids
- prescribing
- chronic pain
- primary care
- cost
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This study focuses on the economic aspects of prescribing opioids in primary care.
This study uses individual patient-level data to quantify opioid prescribing for people with musculoskeletal pain.
This study looks at the coprescribing of opioids in primary care.
This study does not look at longitudinal changes in prescribing opioids to patients with chronic musculoskeletal pain.
This study does not attempt to relate opioid prescriptions with treatment effectiveness.
Introduction
‘Few things a doctor does are more important than relieving pain … pain is soul destroying.’1 These words from Marcia Angell, former editor in chief of the New England Medical Journal, succinctly illustrate the therapeutic need for pain relief. However, prescribers have to balance both benefits and harm to patients from pharmacological treatment. Untreated pain can cause both physical and mental distress. One in five people suffer from chronic pain, the most common sources being back pain (24%) or osteoarthritis (35%).2 3 Findings from the Global Burden of Disease study highlight musculoskeletal conditions as the largest cause of disability in the UK.4 Pain is the main symptom of many musculoskeletal conditions and it is closely associated with depression, anxiety, fatigue and sleep deprivation. The WHO recognises chronic musculoskeletal pain as a global priority and aims to better alert nations to the health and economic costs brought about by musculoskeletal conditions.5
Opioids are a popular form of analgesia. Up to 90% of individuals presenting to pain centres receive opioids.6 There is a lack of evidence supporting the efficacy of opioids for chronic non-malignant pain management. Several studies have demonstrated that opioids achieve negligible improvements in pain, function and quality of life.7–10 In addition, as prescribed doses of opioids increase so does the risk of adverse effects such as depression, anxiety, headaches, insomnia, inadvertent overdose and death.11 According to a UK Office of National Statistics report,12 accidental drug overdose is rising, with the highest number recorded since comparable records began in 1993. Of the 3346 drug poisoning deaths registered in 2014, 53% involved an opiate drug.12 The UK guidelines on chronic pain management for people with low back pain and osteoarthritis13–16 recommend weak opioids as a second-line treatment when the first-line medication (non-steroidal anti-inflammatory drugs, paracetamol or cyclo-oxygenase-2 inhibitors) is ineffective or not tolerated. Strong opioids are to be only prescribed for unremitting cases and even then for short-term use only, stepping patients down to weaker opioids as appropriate, or removing altogether if not effective.15
In past years, there has been a range of publications from both media and the medical profession suggesting that prescribed opioid doses are too high and are prescribed for too long, actually endangering patients.17–19 An editorial in The BMJ entitled: ‘Opioids in the UK: What is the problem?’20 concisely summarised concerns from the growing qualitative literature on the overprescription of opioids for chronic non-malignant pain. There is a growing apprehension that the rise in drug-related deaths parallels a rise in opioid prescriptions.9 21–23 However, this is an argument based on evidence from the USA, where rising numbers of deaths have involved prescription drug overdoses.24–26 There are few reliable data on opioid prescriptions in the UK to infer whether overprescription is an issue.
In this study, our aim was to explore opioid prescribing in a sample of patients with chronic musculoskeletal pain in primary care and to estimate the associated costs. We conducted secondary analyses of prescription data from the COPERS trial: a randomised, multicentre, pragmatic trial of a non-pharmacological group intervention for people with chronic musculoskeletal pain conducted across 27 general practices and musculoskeletal services across the UK.27–29 We undertook a secondary analysis looking at the entire cohort of patients to characterise patterns of opioid prescription and to estimate the opioid prescription cost. We also looked at the regional differences in opioid prescribing between two UK geographical areas —London and the Midlands.
Methods
Data sources and study characteristics
We used an anonymised database from the COPERS trial that contained the prescription data for the 703 participants. Study design, setting and participants' characteristics are described in detail elsewhere.28 29 Briefly, COPERS was a multicentre, pragmatic, randomised controlled effectiveness and cost-effectiveness trial conducted in the UK from 2011 to 2012. Seven hundred and three adults with musculoskeletal pain were randomised using a ratio 1.33:1 to intervention (n=403) or control (n=300). In the intervention group, the participants had usual care and were offered a group self-management intervention using cognitive behavioural approaches for the non-pharmacological management of chronic pain (the COPERS course). The primary outcome was pain-related disability at 12 months (Chronic Pain Grade disability subscale). There was a wide range of secondary outcome measures which included the Hospital Anxiety and Depression Scale, healthcare resource use and EQ-5D-3L. Healthcare resource use data included information on the number of contacts with primary and secondary healthcare services, and prescribing data which were collected from participants’ GP electronic records at 12 months. The study did not find any significant differences in prescribing opioids between the intervention and control groups. No serious adverse events (related or not related to opioid use) were reported in either arm of the trial.29 We therefore conducted cohort analyses using data for both groups to characterise opioid prescribing for people with chronic musculoskeletal pain.
Participants
The characteristics of study participants and recruitment procedures are described elsewhere.27 Briefly, participants were adults (≥18 years) with musculoskeletal pain of at least 3 months’ duration. Causes of pain included, but were not restricted to: osteoarthritis, back pain, chronic widespread pain and fibromyalgia. Participants were recruited in the UK (London and the Midlands) from primary care, community musculoskeletal pain services and secondary care pain services. Exclusion criteria were: inability to give informed consent, not fluent in English, chronic pain arising from active malignant disease or inflammatory arthritis, terminal illness, or serious uncontrolled mental health or substance abuse preventing individuals from participating in the group sessions. The demography of the study participants was: 67% female, mean age 60 years (52 years in London and 67 in Midlands) and 81% white British.
Prescription analysis
We extracted and anonymised prescribing data over 12 months from participants’ GP electronic records. The data set included information on: formulation, dose/strength and the number of prescription items for each participant. A ‘prescription’ refers to a single medicine prescribed by a doctor on a prescription form. The data set contained 40 649 prescriptions in total; these included other items as well as opioids. Opioids were identified in the data set by their generic (non-proprietary) names using the British National Formulary classification system.30 Searches were conducted for strong opioids (buprenorphine, diamorphine, dipipanone, fentanyl, morphine, oxycodone, papaveretum, pentazocine, pethidine, tapentadol and tramadol) and weak opioids (codeine, dihydrocodeine and meptazinol). We also searched for combination formulations which contained weak opioids: co-codamol (codeine phosphate/paracetamol) and co-dydramol (dihydrocodeine/paracetamol). The searches were conducted using wildcards and the VLOOKUP option in Microsoft Excel. The multivariate analysis of variance (MANOVA) was conducted using IBM SPSS Statistics V.22. The cost of opioid prescriptions was calculated using the Prescription Cost Analysis 2012 database31 using a net ingredient cost per item (cost without discount and dispensing fees per single item prescribed on a prescription form). The list of costs used in the study is shown in online supplementary appendix 1. We did not compare oral morphine equivalent doses due to lack of consistency in the conversion ratios taken from different sources.32–34
Supplementary file 1
Results
For the 703 study participants, 413 (59%) were prescribed opioids. In total, 3319 opioid prescriptions were issued over the 12-month period, of which 53% (1768/3319) were for strong opioids (tramadol, buprenorphine, morphine, oxycodone, fentanyl and tapentadol). The number of opioid prescriptions varied from 1 to 52 per person per year. The average number of opioid prescriptions per patient was 8.0 (SD=7.9). Table 1 shows the annual numbers of opioid prescriptions and their costs. The cost per prescription varied from £4 to £63 with oxycodone being the most costly opioid prescription. The overall cost of all prescribed opioids during the 12-month study period was £44 491 (on average £63.29 per participant).
Annual numbers of prescriptions and their costs (n=413)
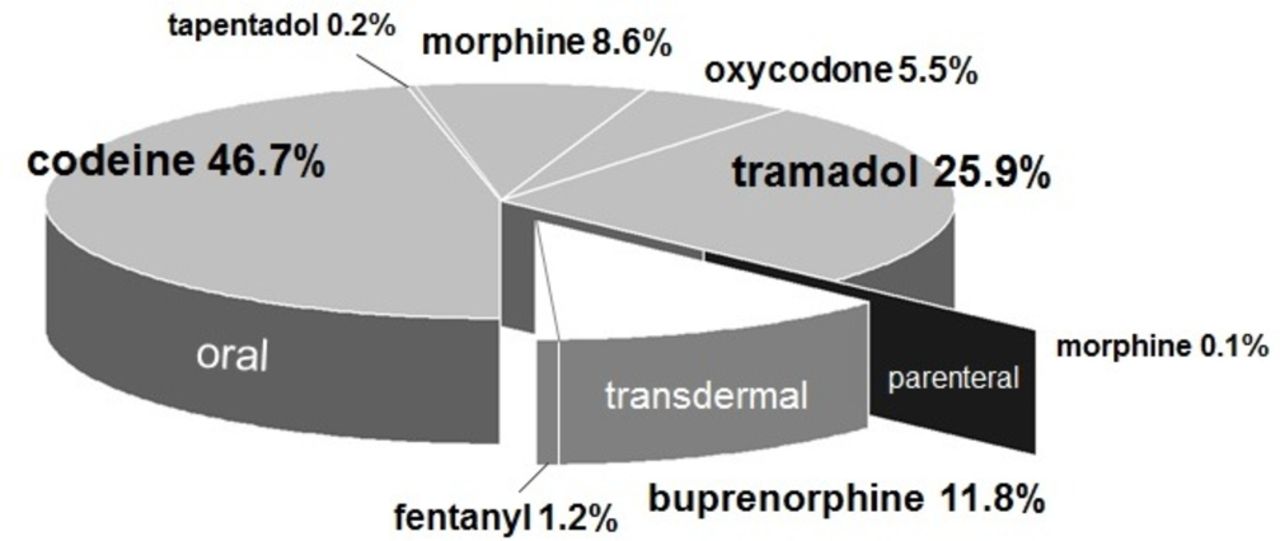
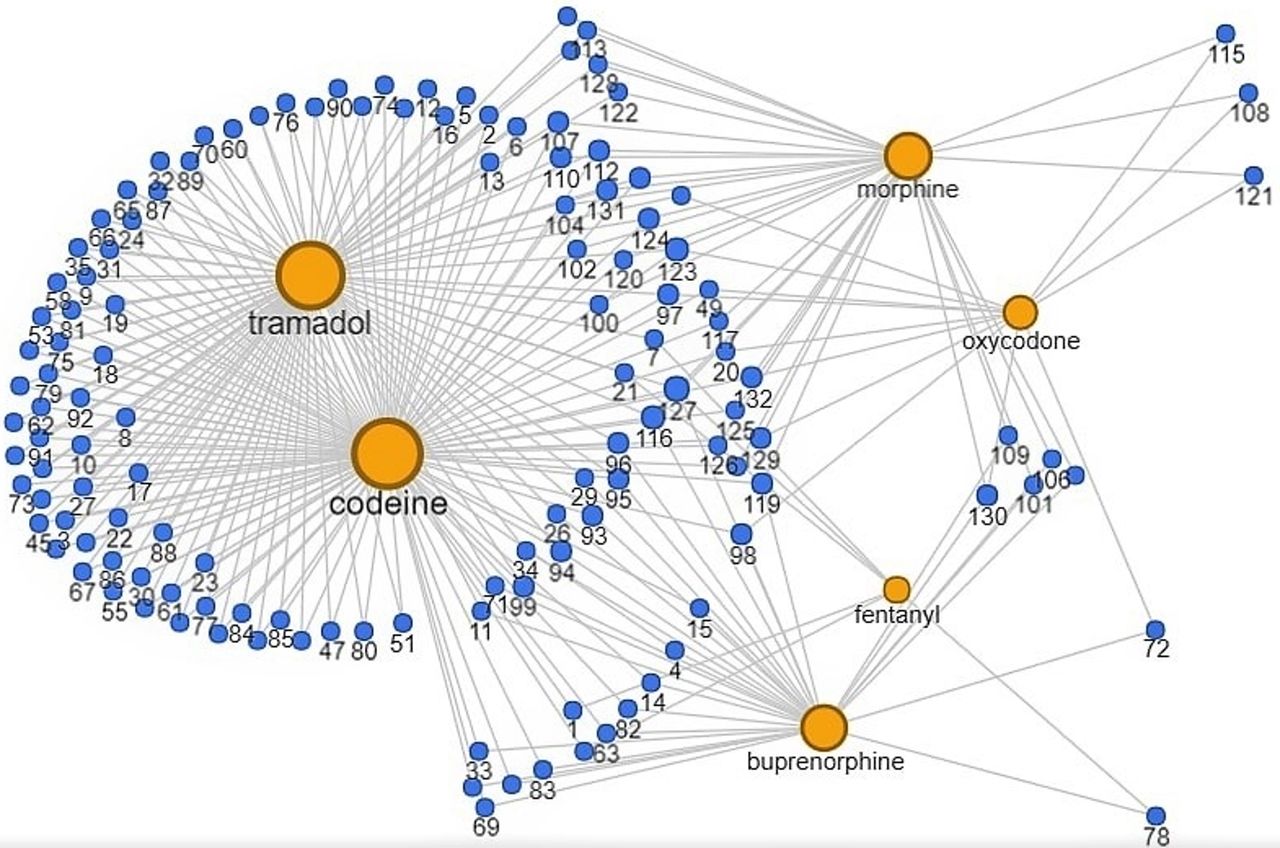
Figure 1 shows the proportions of prescribed opioids. Oral opioids comprised 86.9%, transdermal 13.0% and parenteral 0.1% of all opioids prescribed. The most frequently prescribed opioid was codeine (47%), which also included combination formulations co-codamol (codeine phosphate/paracetamol) and co-dydramol (dihydrocodeine/paracetamol). Tramadol was the most frequently prescribed strong opioid (26%), followed by buprenorphine (12%), morphine (9%) and oxycodone (6%). Parenteral morphine was prescribed to one patient only, although we do know whether this was for chronic pain or for acute pain management. Figure 2 illustrates the coprescribing of different types of opioids in the cohort of patients with chronic musculoskeletal pain. A combination of opioids was prescribed to 32% (132/413) of patients. Among these, 112 (27%) people received two different types of opioids, 17 (4%) three types, and 3 people (1%) were prescribed more than three types of opioids. The most frequent combination of opioids was codeine plus tramadol (83 people), followed by codeine plus morphine (19 people), codeine plus buprenorphine (19 people) and morphine plus tramadol (15 people).

Proportional distribution of opioid prescriptions in the overall cohort of patients.

{kind=link}
{kind=link}
Network plot showing coprescribing of opioids for 132 patients. Patients are indicated by blue circles with numbers, which are linked to prescribed opioids (yellow circles). The size of the circles is proportional to the number of prescribed opioids.
Table 2 summarises numbers of people prescribed different types of opioids in the entire cohort and in the two samples (London and the Midlands). The proportion of people with musculoskeletal pain prescribed opioids was higher in the Midlands sample (63%) compared with the London sample (56%). Morphine was more frequently prescribed in the Midlands (10%) compared with London (3.7%). The average number of opioid prescriptions per patient was also higher in the Midlands sample 8.58 (SD 8.12) compared with the London sample 7.33 (SD 7.56), although this difference was not statistically significant. The proportions of patients receiving different combinations of opioids were similar in the London and the Midland samples. MANOVA tests conducted using prescription numbers for different types of opioids showed no significant differences between London and Midlands samples (p>0.05, not shown).
Number of study participants prescribed opioids and the average number of prescriptions in different samples
Table 3 summarises prescription characteristics for people receiving weak and strong opioids. More than half of these patients (56%, 231/413) were prescribed strong opioids. Patients taking strong opioids received on average 10 prescriptions per year with an annual cost of £174 per patient. Among these people, 40% received >3 strong opioid prescriptions per year, costing on average £236 per person. Patients taking weak opioids received on average five prescriptions a year with an annual cost of £24 per person. Within this group, 21% of people received >3 prescriptions per year costing on average £40 per person.
Characteristics of opioid prescriptions in patients receiving strong and weak opioids (n=413)
Discussion
In this study, we characterised opioid prescribing in a sample of people with chronic musculoskeletal pain recruited from primary care into a trial of a self-management intervention. Opioids were prescribed to 59% of study participants and 53% of these prescriptions were for strong opioids, indicating their frequent prescription for patients with chronic musculoskeletal pain. These strong opioids included tramadol (26%), buprenorphine (12%), morphine (9%) and oxycodone (6%). Approximately 40% of patients received >3 strong opioid prescriptions per year, suggesting long-term prescribing of strong opioids in primary care. According to the national guidelines on chronic pain management for people with low back pain and osteoarthritis,15 16 strong opioids are to be only prescribed in unremitting cases for short-term use, stepping down to weaker opioids, or removing altogether if not effective.15
Currently, there is no accepted definition of overprescribing. The use of this term largely depends on context; it can refer to unnecessary prescription, lack of clinical effectiveness or side effects.35–37 In opioid studies, overprescription is closely associated with opioid misuse and abuse.9 23 38 39 Dunn et al 9 analysed the relationship between prescribed opioid doses and the risk of overdose in 9940 patients with chronic non-malignant pain. People receiving daily oral morphine equivalent doses in the range of 50–99 mg have a 3.7-fold increase in overdose risk, while patients receiving doses of 100 mg or more had an 8.9-fold increase in overdose risk compared with patients prescribed <20 mg/day.9 Given that opioids differ in their potency, formulation and administration routes, converting opioid doses to oral morphine would be one way of identifying the overprescription of opioids. However, there are differences in the conversion ratios to oral morphine used in the national guidelines and formularies.32–34 There is also individual variation in patient response to opioids in terms of metabolism, distribution and receptor dynamics.40 41 Therefore, opioid conversion ratios are purely guidelines that provide starting points for switching between different opioids for the majority of individuals, subject to further assessment and dose titration.
In the context of this study, overprescribing can be defined as the long-term prescribing of strong opioids (>3 prescriptions a year). This is consistent with the National Institute for Health and Care Excellence guidelines for the most common painful conditions (low back pain and osteoarthritis), which recommend strong opioids to be prescribed for a short time only.15 16 We found that 40% of patients receiving opioids for chronic musculoskeletal pain may be overprescribed. The estimated cost of overprescription was £236 per person per year (table 3). According to recent analyses of opioid prescribing in the UK primary care, 1.25–1.38 million people with musculoskeletal conditions receive long-term opioids.42 Assuming that 40% of these people are overprescribed, the cost of opioid overprescription may be over £100 million/year. This does not include costs associated with the management of side effects and overdose. We were unable to calculate these costs since there were no opioid-related serious adverse events in either arm of the trial.29 The trial was not designed to capture non-serious adverse events associated with opioid use.
Although our understanding of chronic pain management has advanced, the effective treatment of chronic pain remains elusive. In the chronic pain management guidelines for Australia, Canada, Germany, USA and UK, weak opioids are considered a treatment option.15 16 43–45 Opioids are used to treat both acute and chronic pain, despite pain experts being in agreement over their poor effectiveness for the latter.46–48 Some reports suggest that prescribing opioids for chronic pain may be associated with poorer functional outcomes (eg, disability, pain intensity, anxiety and depression) compared with other treatment strategies.49 50 Since the late 1990s, under growing public pressure and aggressive pharmaceutical marketing to eliminate pain, physicians globally have been ever more proactive in their efforts to identify and treat chronic pain. In the UK, the latest published data show that from 2005 to 2015 use of analgesics rose by 21 million items, increasing costs by £230.1 million.51 Among opioids, the increase in the number of prescribed items was 10.5% for oxycodone, 9.2% for morphine and 8.9% for buprenorphine.51 Nevertheless, pain intensity does not improve in patients with chronic pain on higher compared with lower opioid doses, indicating poor efficiency in current opioid prescription practice.7–9 Scientific literature is flooded with information on the dangers of opioid misuse, abuse and addiction as a recreational drug.52–54 However, fatalities from recreational opioid misuse are now overshadowed by medically prescribed opioid-related deaths; in the USA, these accounts for 60% of opioid-related deaths,55 and data from the US National Center for Health Statistics show that opioid deaths have increased above that of the deaths from heroin and cocaine combined.24 Physicians have raised the alarm about the rise in opioid prescribing in primary care, saying that in many cases doses are too high and treatments are too long.17–19 56 Current guidelines for the management of conditions associated with chronic pain14–16 reiterate importance of maintaining physical activity, physiotherapy and education programmes. In recent decades, a more holistic approach to chronic pain management has been taken. New treatments involve self-management, coping strategies such as distraction or relaxation techniques, and lower doses of pain relief medication.57 58 The purpose of chronic musculoskeletal pain management is to enable the individual to live with the pain, yet limit its impact on their daily functioning, consistent with a biopsychosocial model of health.59 The cost-effectiveness of these therapies is yet to be established. The study of a non-pharmacological intervention for people with chronic musculoskeletal pain, which generated data for this manuscript, did not find any significant effect on pain severity.28 29 However, the intervention was found to be cost-effective due to a reduction in depression and an improvement in health-related quality of life.28 29 Researchers recognise the importance of assessing multiple outcomes in pain management studies and that research in pain management should go beyond comparing the clinical effectiveness of different treatments, but address questions of ‘what treatment is effective, for which patients, on what outcomes, under what circumstances, and at what cost’.60
Limitations
This study provides a snapshot of opioid prescribing in primary care over a period of 1 year; it did not look at longitudinal changes in prescribing opioids to patients with chronic musculoskeletal pain.
This study focused on the economic aspects of opioid prescribing; it did not attempt to relate opioid prescriptions with treatment effectiveness.
Our analysis assumes that all opioid prescriptions were for chronic pain and not for acute pain episodes.
Conclusions
Long-term prescribing of opioids for chronic musculoskeletal pain is common in primary care. For over a quarter of patients receiving strong opioids, these drugs may have been overprescribed according to national guidelines. The estimated cost of overprescribing opioids in UK primary care may be around £100 million/year.
References
Footnotes
Contributors TA and NH jointly conducted data analysis, wrote the first draft and integrated comments from the coauthors. DC, SJCT, KH, SE, AS, AR, JF and MRU critically revised the manuscript and provided methodological input. NH led data analyses and manuscript production. MRU and SJCT were the principal investigators on the COPERS project. DC, SE, AS and AR were coapplicants on the funding application. All coauthors contributed to the concept of the paper.
Funding This paper presents independent research commissioned by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research scheme (RP-PG-0707-10189).
Disclaimer The views expressed in this publication are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests TA, NH, DC, SJCT, KH, SE, AS, AR and JF have no competing interests with relation to this paper. MRU is an applicant and coapplicant on multiple studies on pain funded by NIHR and ARUK. These include the I-WOTCH trial of opioid reduction 14/224/04 ISRCTN 49470934. He is an editor for the NIHR journal series for which he receives a fee. He is a director and shareholder of Clinvivo.
Patient consent Not required.
Ethics approval Cambridgeshire Ethics Committee provided a favourable ethical review for this study (Ref 11/EE/046).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data available.