Article Text

Abstract
Objectives To conduct a pilot trial of a primary care Symptoms Clinic for patients with medically unexplained symptoms and evaluate recruitment and retention, and acceptability of the intervention and to estimate potential treatment effects for a full trial.
Trial design Randomised parallel group pilot trial.
Setting Primary care in one locality.
Participants Primary care database and postal questionnaire were used to identify patients with multiple specialist referrals and multiple physical symptoms unlikely to be explained by disease.
Interventions General practitioner (GP) with special interest ‘Symptoms Clinic’ + usual care versus usual care alone. The Symptoms Clinic comprised one long (1 h) and three short (20 min) appointments.
Outcomes Number of patients identified and recruited; acceptability of the intervention (items from Client Satisfaction Questionnaire and interview); Medical Outcomes Survey Short Form 12 (SF-12) physical component summary.
Randomisation Automated blocked randomisation accessed by telephone.
Blinding None.
Numbers randomized 16 to intervention and 16 to usual care alone.
Recruitment 72 patients, from seven GP practices, had repeated specialist referrals and a Patient Health Questionnaire (PHQ)-15 score of ≥10 indicating a high probability of medically unexplained symptoms. 15 were ineligible and 25 declined to participate.
Numbers analysed 26 patients; two patients randomised to the intervention group were incorrectly included, three patients in the intervention group and one control did not complete outcome measures.
Outcome Most patients randomised to the Symptoms Clinic found the intervention acceptable: eight out of 11 reported the intervention helped them to deal with their problems. The mean difference between groups in SF-12 physical component summary, adjusted for baseline, was 3.8 points (SD 6).
Harms No observed harms.
Conclusions Patients with multiple medically unexplained symptoms can be systematically identified in primary care; a randomised trial comparing the Symptoms Clinic with usual care is feasible and has the potential to show clinically meaningful benefit.
Trial registration ISRCTN63083469.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
There are few effective non-specialist interventions for patients with multiple medically unexplained symptoms in primary care.
We developed a new general practitioner (GP) with special interest ‘Symptoms Clinic’ and carried out a pilot randomised trial.
The pilot trial aimed to test the systematic identification of eligible patients, assess the acceptability of the intervention and estimate potential treatment effects for a larger trial.
Key messages
Patients with multiple medically unexplained symptoms can be identified systematically from the primary care database and a symptom questionnaire.
The Symptoms Clinic appears to be an acceptable model for patients.
A larger trial using these methods is feasible.
Strengths and limitations of this study
This study was carried out by one GP with special interest in medically unexplained symptoms. Further work to demonstrate transferability of the clinic model is needed before a larger trial.
Introduction
Physical symptoms that cannot be adequately explained by organic pathology are common in both primary and secondary care.1 2 For some patients (approximately 1% of the population), the number, persistence or intrusiveness of these so-called medically unexplained symptoms (MUS) leads to repeated consultation, referral for investigation and impaired quality of life.3 4 Patients with MUS, who have been repeatedly referred to specialists, have impaired physical and mental health and incur substantial health costs with little apparent benefit.5
There is evidence for the efficacy of intensive treatment of severe MUS with cognitive behavioural therapy delivered by specialists.6 7 Specialist psychiatric consultation followed by a management planning letter has been found to offer only modest benefit.8 Trials of teaching general practitioners (GPs) to use brief interventions such as reattribution in routine consultations have failed to show consistent benefit.9–11 All these approaches concentrate on making the link between physical symptoms and underlying psychological cause. An alternative approach is to initially provide conventional biomedical explanations for MUS12 13 and to only embark on psychosocial talk when cued by the patient.14
We have developed a primary care Symptoms Clinic for patients with multiple MUS, which comprises a structured set of consultations with a specially trained GP with special interest. The GP explores acceptable explanations for symptoms in terms of biological (including neurological and cognitive) mechanisms rather than psychological cause, provides empathic support and then helps patients to address specific symptom-maintaining factors by medication or with cognitive behavioural techniques. Here, we describe a pilot randomised controlled trial, which compared this Symptoms Clinic as a supplement to usual care with usual primary care alone.
The aim of this study was to determine the feasibility of conducting a larger trial of the Symptoms Clinic. We examined the following components of feasibility: systematic identification of patients, trial recruitment and retention, acceptability of the Symptoms Clinic intervention and a preliminary estimation of potential treatment effects.
Methods
The study was conducted in Edinburgh between August 2009 and May 2010. Participating practices took part in identifying potential patients, and the trial clinics were held in an outpatient clinical treatment facility. The study had approval from Lothian Research Ethics Committee (reference 09/S1102/34) and was registered (reference ISRCTN63083469).
Trial design
This was a pilot trial using an individually randomised parallel group design with patients allocated equally to intervention and control arms. The trial was conducted with no major alterations to the initial protocol.
Participants
Eligible patients comprised adults aged 18–65 years and registered with participating practices who met all the three criteria: (1) they had been referred at least twice to specialists in the preceding 3 years, (2) they currently reported multiple physical symptoms and (3) their GP believed that their symptoms were unlikely to be adequately explained by physical disease. These criteria were identified sequentially.
In the first stage, practices carried out a computerised search of medical records to identify patients aged 18–64 years who had been referred at least twice to hospital outpatient clinics in the preceding 3 years, did not have a diagnosis of serious illness (coronary heart disease, stroke, cancer, severe mental illness) and had one or more diagnostic codes potentially indicating MUS. All diagnostic codes are listed in online appendix 1. As a pilot of this primary search strategy (search A) in two additional practices returned fewer individuals than expected due to low rates of coding for MUS, we added a secondary search (search B) that required three or more referrals but no codes for MUS. Searches were developed specifically for this study (Campbell Software Solutions) to run on the GPASS clinical system.
Current physical symptoms were assessed in patients identified by the search for referrals by postal questionnaire. This included the Patient Health Questionnaire (PHQ)-14, a modified version of the PHQ-15 scale15 in order to identify patients with multiple physical symptoms, which are commonly medically unexplained. We omitted the item about menstrual symptoms because the study population included men and older women. Before sending these, the practice GPs checked the list of names to avoid sending the questionnaire to patients who were seriously ill or for whom it would be clearly inappropriate. The postal PHQ-14 was accompanied by an information sheet. We defined multiple physical symptoms as a score of ≥10 on the PHQ-14, indicating at least moderate severity of MUS.15 The likelihood that current symptoms could not be explained by physical disease was assessed by asking the GPs to review the casenotes of all patients who returned the questionnaire with a PHQ-14 score of ≥10 and indicated an interest in taking part in the trial. The GPs were also asked to exclude patients who were unable to leave the house independently, or for whom other health or social problems precluded an invitation to take part in a study. Additional exclusion criteria were assessed during the baseline assessment and were as follows: patient reported thoughts of self harm more than a few times in a week (an item in the PHQ-9), current self-reported alcohol or drug problems and either current or planned engagement in psychological treatment.
Baseline assessment and consent
The researcher (WM) carried out baseline assessment and obtained informed consent during an interview. Baseline measures included: age, sex and current occupation; physical symptoms, assessed using the PHQ-14; health status by Medical Outcomes Survey Short Form 12 (SF-12) physical and mental component summaries; depression by PHQ-916 and anxiety by General Anxiety Disorder 7 Questionnaire (GAD-7).17
The general practice records (paper and electronic) of all participants were reviewed by the researcher in order to record patients' prior use of both primary and secondary healthcare services. This was done in order to provide a baseline measure, but in view of the short duration of this pilot trial, it was not repeated as a follow-up measure. The number of consultations in the preceding year and referrals in the preceding 3 years were recorded, and the number of consultations and referrals attributable to probable MUS were estimated using a method based on the contents of the record entries.18
Randomisation
Following completion of the baseline assessment, patients were randomised to either usual care or intervention (usual care + the Symptoms Clinic) by the researcher. Randomisation was carried out by automated telephone system using blocked allocation with variable block size.
Usual care
Patients in both arms continued to receive usual care from their registered general practice. This included referral for investigation or treatment of symptoms as the GP deemed appropriate.
Symptoms Clinic
Patients allocated to the Symptoms Clinic were offered four appointments; the first was of 1 h duration and the subsequent three lasted 20 min. All consultations were at the treatment centre, and patients were seen by the same doctor (CB), an experienced GP with special interest in MUS. The consultations were structured to first hear the patient's experience of illness then to propose and negotiate constructive explanations of physical symptoms. These explanations were used as the basis for simple cognitive and behavioural actions to modify symptoms and their impact. No specific attempt was made to screen for common mental disorders; however, patients were encouraged to describe their emotional responses to symptoms and other events, and diagnostic labels such as depression were discussed collaboratively with the patient rather than imposed by the doctor.
Outcome measures
Outcome measures were chosen to measure four components of feasibility: systematic identification of patients, trial recruitment and retention, acceptability of the Symptoms Clinic intervention and estimation of potential treatment effects.
The systematic identification, recruitment and retention of trial participants was assessed by documenting the numbers of patients at each stage of the study and by checking that their baseline characteristics were similar to those seen in our epidemiological study of patients repeatedly referred with MUS.4 5
The acceptability to participants of the Symptoms Clinic patients was measured by administration of a Client Satisfaction Questionnaire and by asking all patients who had attended the clinic to participate in a brief interview to determine their experiences of the study procedures and the Symptoms Clinic. We noted the number of eligible patients who declined to enter the trial. We also followed-up patients who dropped out of the trial in order to ascertain the reason for this. This follow-up was carried out by telephone on two occasions and then by letter from one of the investigators who had no involvement with day-to-day contact of the trial. In order to estimate likely treatment effects, we repeated the following scales from baseline: PHQ-14, SF-12, PHQ-9 and GAD-7. In addition, patients completed the Patient Global Impression of Change. These measures were obtained by postal questionnaire (with telephone follow-up of non-responders) 12 weeks after randomisation.
Sample size and statistical analysis
For this pilot trial, we aimed to randomise approximately 30 patients in order to obtain a reasonable range of clinical conditions and test the clinic and trial procedures adequately. The effects of the intervention were estimated using analysis of covariance with baseline value as a covariate.
Results
All 15 practices in north-east Edinburgh were invited to take part. The population of this urban area is socioeconomically diverse. Nine of the practices currently used the GPASS clinical database on which the search was run and six agreed to take part. We subsequently recruited one additional practice. The total number of patients registered with the seven practices was 45 064.
Patient identification and recruitment
The database searches identified 863 patients (1.9% of the total general practice population), and questionnaires were sent to a randomly selected 486 of these. One hundred and five patients (21.6%) responded and 72 of these had a PHQ-14 score of ≥10. GPs deemed 10 of these patients ineligible, and a further 22 were unable to attend the baseline assessment. Five patients were excluded at baseline assessment because of thoughts of self-harm, and a further three failed to attend, leaving 32 who were randomised to either usual care or the Symptoms Clinic plus usual care. These data are summarised in figure 1.

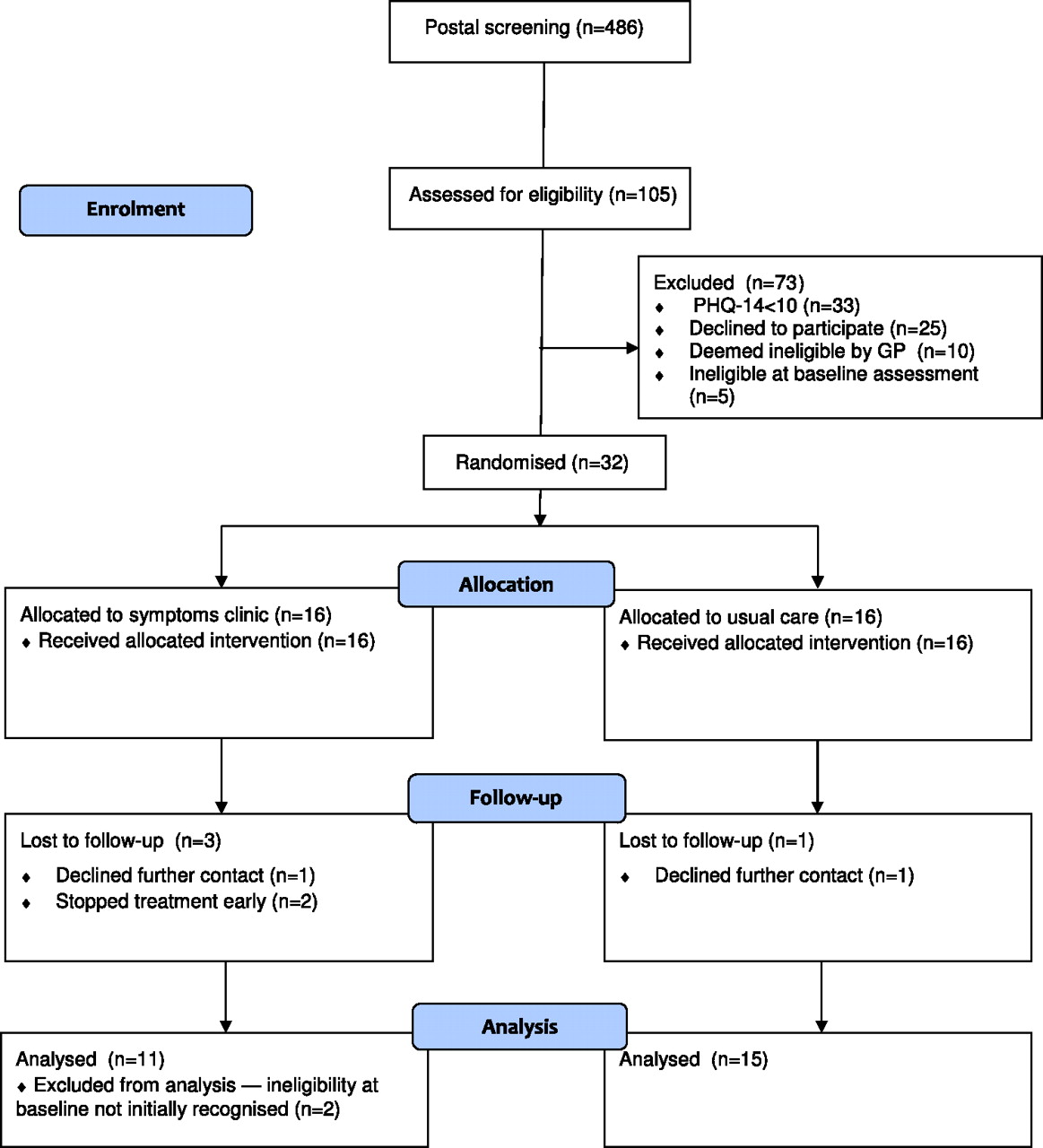{kind=link}
Flowchart for Symptoms Clinic Pilot Trial.
The number of patients identified by the search A was smaller than anticipated, probably reflecting low rates of coding for MUS syndromes within practices. However, when we used the criterion of three or more referrals without requiring any specific MUS syndrome (search B), it identified three patients who on clinic assessment had localised joint pain as their main symptom. While these patients also reported other symptoms on the PHQ-14, it was the localised joint pain, which had the greatest effect on their functioning. As patients saw addressing the joint pain (in one case surgically) as their top priority, the Symptoms Clinic model was less appropriate than for patients who were still seeking an explanation for their symptoms.
Patients' characteristics
Baseline measures are shown in table 1. Patients had substantially impaired physical and mental health status: scores on the SF-12 Physical Component Summary are standardised to population norms with mean and SD of 50 and 10, respectively, and these results placed the participants in the lowest decile of the general population, despite the absence of physical disease. Around half the participating patients had comorbid anxiety or depression. Participants were high users of health services: they had a mean (SD) of 27 (11) GP consultations and 4.7 (1.8) specialist referrals over the preceding 3 years, of which 15 consultations and 3.4 referrals were estimated from the records to be for MUS.
Baseline measures by allocation group
Trial retention and acceptability of clinic model and procedures
All 16 patients randomised to the Symptoms Clinic attended the first appointment and 11 completed either three or four appointments. Of the remainder, two were clearly improving at the time they were seen and agreed to early discharge; two found further attendance difficult after a second appointment and one declined any further contact after the first appointment. Several patients randomised to usual care expressed some disappointment at the time of their allocation, although follow-up response rates were comparable between the two groups.
Responses to the Client Satisfaction Questionnaire from patients randomised to the Symptoms Clinic suggested that the process was acceptable: eight out of 11 reported that it helped them to deal with their problems more effectively. Interviews suggested that most patients appreciated the time and the explanatory approach adopted by the Symptoms Clinic. A few remained sceptical, indicating that they felt that the aim was simply to assert that their problems were psychological, but most seemed comfortable with the balance between psychological and physical components taken by the clinic. There were few reported problems with the trial procedures among participants.
Practices reported experiencing no major problems with the process for identifying or recruiting patients. The searches took <30 min; and the checking of the resulting patient lists for those who were ineligible was also quick and straightforward as patients were often well known to the doctors.
Estimates of potential treatment effects
Outcome measures were obtained for 28 (84%) patients. No follow-up data were available, despite repeated requests from four patients, three in the intervention group and one in usual care. Two of the non-responders had predominantly musculoskeletal pain and would not have been included in the search strategy, which required one or more MUS syndrome diagnoses. Two patients whose postal PHQ-14 had been above the entry threshold of 10 but whose baseline PHQ-14 score was below 10 were entered into the study in error and randomised to the Symptoms Clinic. Because this ineligibility was recorded before randomisation but not recognised at the time, they were excluded from the analysis.
Outcome measures are summarised by group in table 2. For the SF-12 component scores, higher scores represent better health; for PHQ-14, PHQ-9 and GAD-7, higher scores represent worse health. The Patient Global Impression of Change showed an improvement of one or more levels in seven of 11 patients in the Symptoms Clinic arm and two of 15 in the usual care arm. Table 2 includes no measures of statistical significance, given the small sample size, it does, however, include the SD of the residuals from the fitted analysis of covariance models. Based on these, a difference in outcomes between groups of two points in the PHQ-14 and three points in the SF-12 Physical Component Score would represent effect sizes of around 0.5 times the SD. Although we are not aware of studies assessing clinically important difference with these scales in a comparable population, a standardised effect size of 0.5 is generally found to represent a clinically meaningful difference.19 We did not measure subsequent healthcare use in this short-term pilot study but regard this as an important outcome for future studies.
Outcome measures at baseline and follow-up by intervention group
Discussion
Summary of main findings
This pilot trial supports the feasibility of conducting a trial of the Symptoms Clinic. The trial procedures, including identification, recruitment and randomisation were acceptable to patients. Nonetheless, a few patients were lost to follow-up and further attention to the entry criteria is warranted. The trial was not powered to detect treatment effects, but the results were in keeping with clinically meaningful benefit.
Strengths and limitations
This study design had several strengths, particularly in relation to identifying potential patients. Systematic identification of patients that combines high healthcare use (referrals) with multiple symptoms on self-report has not been used before but is in keeping with the defining features of patients with MUS.20 The search methods for this study were similar to our previous epidemiological work4 5 using a database, however, whereas previously we carried out detailed casenote review to identify patients, in this study, we combined repeated referrals with a high self-reported symptom count. We found that the health-related quality of life and prevalence of depression and anxiety in patients recruited into this pilot study were similar to those in our previous descriptive study of a similarly defined patient sample.4 5 This suggests that the sampling method used in the trial achieved a representative sample. In a future trial, other outcome measures could be considered: in particular, a measure of healthcare use. The small scale of this study is not a limitation of this pilot study, which was designed to test procedures rather than reach conclusions about effect.21
Comparison with other recruitment and intervention strategies
Previous studies of primary care interventions for patients with MUS have depended on either questionnaire sampling,9 GP identification and referral8 or review of consultations by investigators to decide whether symptoms were medically unexplained.10 All these have limitations for identifying patients with MUS and high healthcare use. Only one trial has used systematic searching of clinical records; this was a lengthy process carried out by hand.18 The recruitment strategy we used had the advantage of combining activity data from electronic records (referrals and diagnostic coding) with symptoms reporting on questionnaire.
Although there have been policy statements advocating intermediate care services for patients with MUS,22 there have been no formal studies of this approach. The model here differs from conventional approaches: it is much shorter than cognitive behavioural therapy but longer and less psychologically oriented than reattribution. Recent evidence suggests that patients often actively resist reattribution.23 Even when they have anxiety and depression, patients with MUS may see them as associated with rather than causal to their physical symptoms.24 Unlike the consultation letter approach, the Symptom Clinic model aims to negotiate a ‘medical’ explanation for symptoms involving physiological processes, thus reducing uncertainty and permitting an exit from the diagnostic cycle.25 This explanation is then followed up over a series of shorter consultations.
Implications for future research
This pilot study has identified an effective method for systematically identifying patients in primary care who have MUS and relatively high use of secondary care. Further work is now needed to better understand patients' views, of which aspects of the intervention were most helpful and to protocolise a final version of the intervention before undertaking definitive tests of its efficacy. Providing that the Symptoms Clinic model can be shown to be delivered consistently by a range of doctors, it offers a novel approach to a common problem that warrants testing in a full-scale trial.
Conclusions
We found that the Symptoms Clinic intervention, and the trial procedures we used to test its efficacy, were acceptable to patients. Given the prevalence of MUS and their cost to health services, treatments are required that can be effectively delivered in primary care, need limited amounts of time per patient and can be taught relatively quickly. The Symptoms Clinic meets these requirements and now requires further evaluation.
Acknowledgments
We acknowledge the support and cooperation of Dr Jane Walker in designing the trial, participating practices and the staff of Leith Community Treatment Centre.
References
Footnotes
To cite: Burton C, Weller D, Marsden W, et al. A primary care Symptoms Clinic for patients with medically unexplained symptoms: pilot randomised trial. BMJ Open 2012;2:e000513. doi:10.1136/bmjopen-2011-000513
Contributors CB conceived and designed the study in collaboration with MS, DW and AW; WM collected the data. CB drafted the paper with contributions from all authors. All authors approved the version submitted for publication.
Funding The study was funded by Chief Scientist Office (reference CZG/2/412).
Competing interests None.
Ethics approval Ethics approval was provided by South East Scotland REC.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There is no additional data available.