Article Text

Abstract
Objectives To examine whether the introduction of intermittent standing bouts during the workday using a height-adjustable workstation can improve subjective levels of fatigue, musculoskeletal discomfort and work productivity relative to seated work.
Methods Overweight/obese office workers (n=23; age 48.2±7.9 years, body mass index 29.6±4 kg/m2) undertook two, 5-day experimental conditions in an equal, randomised (1:1) order. In a simulated office environment, participants performed their usual occupational tasks for 8 h/day in a: seated work posture (SIT condition); or interchanging between a standing and seated work posture every 30 min using an electric, height-adjustable workstation (STAND-SIT condition). Self-administered questionnaires measuring fatigue, musculoskeletal discomfort and work productivity were performed on day 5 of each experimental condition.
Results Participants’ total fatigue score was significantly higher during the SIT condition (mean 67.8 (95% CI 58.8 to 76.7)) compared with the STAND-SIT condition (52.7 (43.8 to 61.5); p<0.001). Lower back musculoskeletal discomfort was significantly reduced during the STAND-SIT condition compared with the SIT condition (31.8% reduction; p=0.03). Despite concentration/focus being significantly higher during the SIT condition (p=0.006), there was a trend towards improved overall work productivity in favour of the STAND-SIT condition (p=0.053).
Conclusions Transitioning from a seated to a standing work posture every 30 min across the workday, relative to seated work, led to a significant reduction in fatigue levels and lower back discomfort in overweight/obese office workers, while maintaining work productivity. Future investigations should be directed at understanding whether sustained use of height-adjustable workstations promote concentration and productivity at work.
Trial Registration Number ACTRN12611000632998.
- sedentary behaviour
Statistics from Altmetric.com
What this paper adds
-
Too much sitting is known to be associated with increased health risk; office workers can be exposed to prolonged and uninterrupted sitting time.
-
The use of height-adjustable workstations to promote intermittent standing is shown to reduce postprandial glucose levels; whether reducing sitting time with standing bouts can influence fatigue, musculoskeletal discomfort and productivity is not known.
-
We observed a reduction in all aspects of fatigue and musculoskeletal discomfort in the lower back, but no significant impact—either positive or negative—on productivity, when replacing 4 h of occupational sitting with 4 h of standing each workday.
-
Our results suggest broader benefits of regular standing breaks across the workday, showing reductions in fatigue and musculoskeletal discomfort without impacting on productivity, relative to seated work.
-
These findings complement the body of evidence that height-adjustable workstations can help to reduce workplace sitting time–showing potential beneficial impacts on aspects of worker well-being.
Introduction
Recent guidelines from leading health agencies in Australia1 and the UK2 have provided explicit recommendations relating to reducing sedentary behaviour for preventive health benefits. Specifically, they advocate that adults (18–64 years) should limit the amount of time they spend sedentary and increase the number of breaks during prolonged sitting.
Office workers are one occupational group who are particularly vulnerable to prolonged and uninterrupted sedentary behaviour.3 ,4 As modern workplace environments become increasingly dependent on computer use, the challenge that exists from a public health perspective is how best to alter office workers’ postural allocations during the day to be less reliant on prolonged sitting.
Previous research in which prolonged sitting has been periodically interrupted with short bouts of treadmill walking has shown benefits for cardiometabolic health.5 ,6 However, the practicality and potential impact on work productivity makes it difficult to implement this broadly in an office setting. Several recent interventions have investigated the feasibility of using height-adjustable workstations to reduce workplace sitting time and have shown that they facilitate small behaviour changes, predominately in the form of increased standing time.7–10
Height-adjustable workstations that allow workers to transition seamlessly between a seated to an upright posture have historically been used by workers with long-standing health problems11 or in ergonomic studies to reduce the incidence of musculoskeletal disorders in highly repetitive, sedentary occupations.12–14 Short-duration work tasks that require alternating between sitting and standing postures have also been shown to reduce monotonous feelings of fatigue15 and musculoskeletal exposure.16 This is possibly because a ‘combination of postures’ helps to lower the chronic static work load that can be placed on postural muscles, compared with constant sitting or standing postures.
Two recent studies performed under controlled16 and free-living8 conditions compared the use of a height-adjustable workstation with a traditional workstation and found that workers who modestly reduced their occupational sitting time (40–66 min per workday) also reported improved upper body musculoskeletal symptoms, task accuracy, productivity and mood; whether similar effects would occur from greater reductions in occupational sitting time is unclear.
There is the potential to implement workplace policy changes to reduce sedentary time to improve health through the introduction of height-adjustable workstations. In this context, the next logical step is to better understand, through a well-controlled laboratory study, what effect replacing substantial occupational sitting time (i.e. 50% of the workday) with standing has on measures of fatigue, musculoskeletal symptoms and productivity.
We examined the short-term (5-day) effect of replacing workplace sitting time with routine 30 min bouts of standing on subjective levels of fatigue, musculoskeletal discomfort and work productivity in overweight/obese, but otherwise healthy, office workers. It was hypothesised that the routine introduction of standing bouts across the workday using an electric, height-adjustable workstation would reduce fatigue and musculoskeletal symptoms in office workers without adverse effects on work productivity.
Methods
Participants
Participants were recruited as part of the Sit or Stand @ Work Study that has been described previously.17 Briefly, 17 men and 6 women who were overweight/obese (mean±SD body mass index (BMI) 29.6±4.1 kg/m2), middle-aged (mean age 48.2±8 years) and employed full-time in habitually sedentary occupations (73.9% office workers) were recruited from the general community. Adults were excluded from the study if they sat <4 h/day at work, were pregnant, non-English speaking or had a pre-existing musculoskeletal injury. All adults provided written informed consent and all received financial compensation for their time at the conclusion of the study.
Study design
Details of the main Sit or Stand @ Work Study design and primary outcomes have been described in detail elsewhere.17 The study involved an equal randomised (1:1), controlled, cross-over design with two short-term experimental conditions.
Experimental conditions were performed over 5 consecutive workdays (Monday to Friday) with a minimum 7-day washout period between to eliminate any potential carryover effects (median 7 days, range 7–35; 61% had a 7-day washout period). During the conditions, participants were asked to perform their usual computer and/or telephone-based work tasks in a simulated office setting for 8 h/day in either a seated work posture (SIT condition) or while systematically interchanging every 30 min between a standing and seated work posture (STAND-SIT condition).
The simulated office setting included standard office equipment (telephone, computer, internet access) and an electric, height-adjustable workstation (model 1600×800 mm, Linak, Australia) with an adjustable table height of 665–1340 mm. Participants were provided with a timer to prompt them to adjust the height of the workstation (up or down) every 30 min during the STAND-SIT condition. For consistency, participants preprogrammed the height of the workstation for standing bouts. The study is registered with the Australian New Zealand Clinical Trials Registry (ACTRN12611000632998).
Experimental protocol
Prior to the start of the first experimental condition, participants were given brief verbal instructions on how to adjust the computer monitor and work surface of the height-adjustable workstation in order to maintain a correct ergonomic work posture.
For each condition, participants arrived at the laboratory between 07:00 and 09:30 am to start their 8 h workday. To ensure protocol compliance, participants were directly observed during work hours and asked to wear an activPAL3 tri-axial physical activity monitor (PAL-technologies Ltd, Glasgow, Scotland) on their right thigh to record time spent sitting/standing/walking. Light-ambulatory movement was only permitted within the confines of the laboratory during periods of standing (STAND-SIT condition only) or to go to the toilet (both conditions).
On day 5 of each experimental condition (at ∼1300), participants completed a set of self-administered questionnaires. The questionnaires asked participants to recall behaviour from the past 5 workdays only and included: the Individual Strength (CIS20-R) Questionnaire, Multidimensional Assessment of Fatigue (MAF) Scale, Modified Standardised Nordic General Questionnaire and the Health and Work Questionnaire (HWQ). Workstation acceptability was also assessed using a visual analogue scale (VAS) during each experimental condition. Participants were free to leave the laboratory after the completion of the questionnaires.
Outcome measures
Assessment of fatigue
Fatigue was assessed using a modified version of the Individual Strength (CIS20-R) Questionnaire and the MAF Scale. The CIS20-R is a validated, multidimensional questionnaire that measures total fatigue as well as four subscales of fatigue: subjective feeling of fatigue, reduction of motivation, reduction of physical activity and reduction of concentration. The questionnaire contained 20 statements and was adapted to assess fatigue experienced during the past work week only. Participants were asked to score each statement on a 7-point Likert scale (1=yes, i.e. true, to 7=no i.e. not true). As previously described,18 the questionnaire has a high internal reliability (Cronbach's alpha coefficient for total fatigue is 0.9; and for subscales ranges from 0.83 to 0.92) and is valid for use in the working population.19 Methods of scoring total fatigue and the four subscales have been described in detail elsewhere.19 Briefly, the total fatigue score is derived from the sum of the four subscale scores; a total score >66 was used to indicate elevated fatigue as this score is one SD above the mean score that has been observed in healthy white-collar workers.19 When assessing the four subscales, higher scores indicated a higher degree of fatigue, increased concentration problems, reduced motivation and decreased levels of physical activity.
The MAF Scale required participants to reflect on their fatigue patterns over the past week to derive a Global Fatigue Index (MAF-GFI). The questionnaire contained 16 items, of which 14 used a 10-point Likert scale (1=not at all and 10=a great deal) and two had multiple choice responses. The questionnaire has high internal consistency (Cronbach's alpha=0.93) and is valid for use in a variety of patient cohorts including healthy adults.20 The MAF-GIF was derived from items 1–15 and the scale ranged from 1 to 50, with a higher score indicating greater fatigue severity. As there is no predefined score for clinically significant fatigue, a MAF-GIF score of ≥30 was selected as it is one SD above the mean score that has been observed in healthy controls.20
Assessment of musculoskeletal discomfort
A modified version of the Standardised Nordic Questionnaire for the analysis of general musculoskeletal symptoms was used by participants to indicate areas and severity of pain/discomfort during each experimental condition. Briefly, the questionnaire presented a diagram of the human body (as viewed from the back) that had been divided into nine clearly marked anatomical regions (neck, shoulder, elbow, hand/wrist, upper back, lower back, hip/thigh, knee and ankle/foot). The nine anatomical areas were selected on the basis of two criteria: regions where symptoms tend to accumulate and regions that are distinguishable from each other.21 Participants were asked to indicate by selecting an appropriate response box whether they had discomfort in the indicated areas at any time during the preceding 12 months and during the past five workdays of the experimental condition (modified from past 7 days). If during the past 5 workdays participants experienced discomfort in an indicated area they were additionally asked to nominate (via Yes or No response) whether it had affected/prevented them from performing their work tasks. The Standardised Nordic General Questionnaire has an acceptable level of variance21 and has been validated for use in a variety of occupational groups including computer and call centre workers.22 ,23
Assessment of work productivity
A modified version of the HWQ (available from http://tc.bmjjournals.com/cgi/data/10/3/233/DC1/1) was administered to assess several subscales of workplace productivity including: overall productivity, impatience/irritability, concentration/focus and work satisfaction. The HWQ contained 24 items, several of which were multipart questions. Each item had a tailored 10-point response scale, where: 1=very dissatisfied to 10=very satisfied, for questions dealing with work satisfaction; and 1=my worst ever to 10=my best ever, for questions rating quantity, quality and efficiency of work. Details for scoring the questionnaire have been described elsewhere.24 Briefly, scores for individual subscales were derived by averaging items within the subscales, with a higher score indicative of improved workplace productivity. The HWQ has been shown to have very good internal consistency reliability (coefficient alpha range for scales: 0.84–0.96), with the exception of impatience/irritability, which demonstrates adequate reliability (0.72). The questionnaire has also been shown to be valid against objective measures of productivity in the workplace.24 Copyright of the HWQ is owned by the GlaxoSmithKline Group of companies (@2000).
Assessment of height-adjustable workstation acceptability
Workstation acceptability during the experimental conditions was assessed using a 10 cm VAS reported in millimetres (i.e. scale ranged from 0 to 100 mm with 0 mm=‘Not at all’ and 100 mm=‘Extremely’). Participants were asked to quantify how much they enjoyed using the electric, height-adjustable workstation over the past 5 workdays by drawing a vertical line at a point on the 100 mm scale.
Statistical analyses
All statistical analyses for outcome measures were performed in STATA V.12.0 for Windows (StataCorp LP) using a two-tailed probability level of 0.05. Linear and logistic mixed models adjusting for order effects were used to examine between condition differences in self-reported questionnaire measures. Participants were treated as random effects in these models. Study participants with a missing value for a particular measure were excluded from the analysis of that measure (i.e. participant data were excluded only from the experimental condition that contained the missing value); no missing values were imputed. McNemar's test for dependent proportions was used to determine significant changes (expressed as a %) in the prevalence of musculoskeletal symptoms between experimental conditions. ActivPAL3 tri-axial physical activity monitor data collected in 15 s epochs were analysed using SAS V.9.3.1. Data are reported as mean±SEM or marginal mean±95% CI in the text and tables unless otherwise indicated.
Results
Of the 23 study participants who completed the study, 15 were classed as overweight (mean BMI (SD): 27.54 (1.4) kg/m2) and 8 were clinically obese (mean BMI (SD): 33.7 (4.3) kg/m2); all reported sitting at work for an average of 6.6±1.2 h/day. Protocol compliance during the two experimental conditions was high (SIT-condition: 468.1±1.3 min sitting, 3.2±0.4 min stepping and 7.9±0.8 min standing per 8 h workday; STAND-SIT condition: 232±1.4 min sitting, 5.6±0.4 min stepping and 242.5±1.5 min standing per 8 h workday).
Differences in self-reported fatigue levels
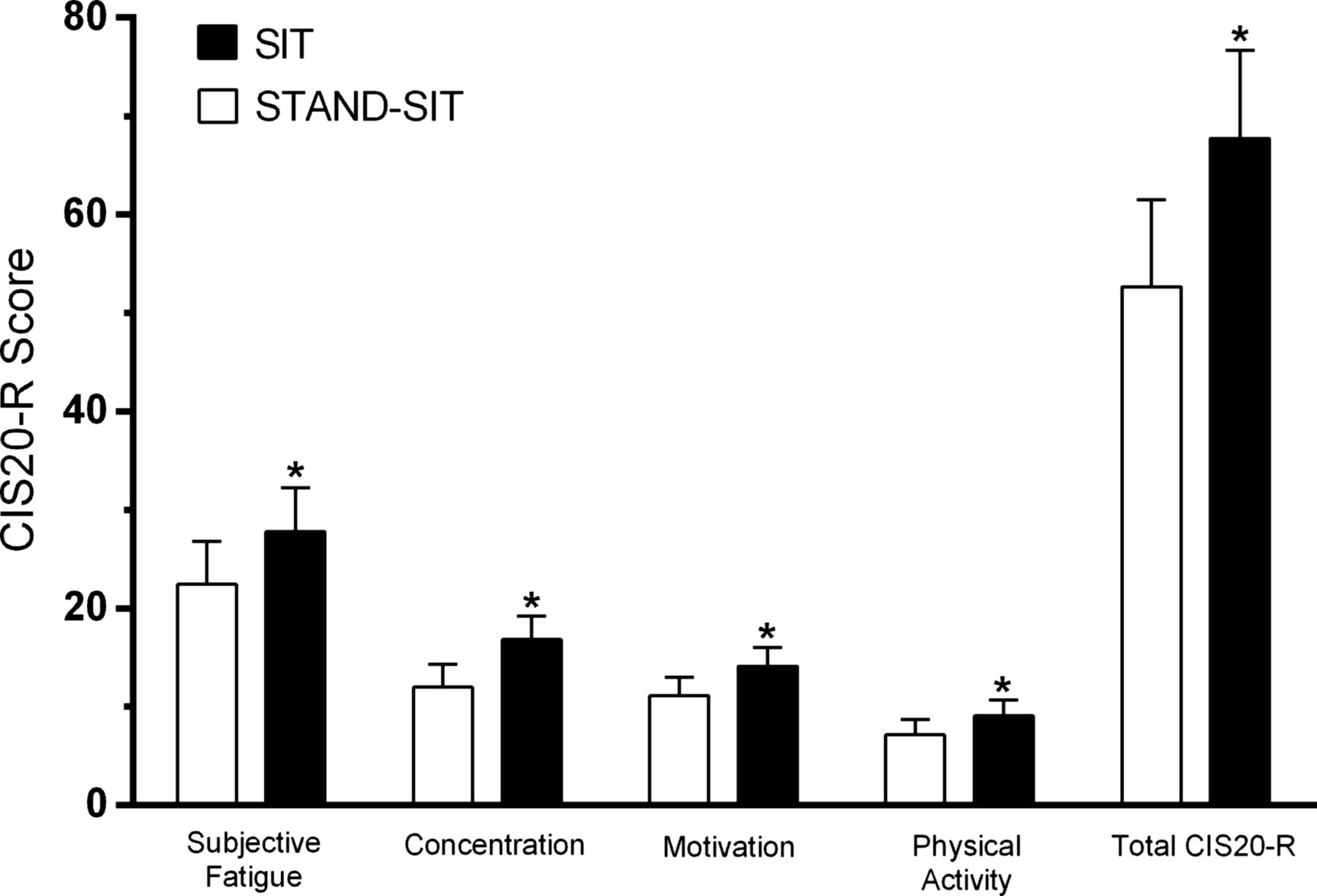
As shown in figure 1, significant differences were observed between conditions for all measures of fatigue based on the CIS20-R Questionnaire (all p<0.007). Participants’ total fatigue score was significantly higher during the SIT (mean 67.8 (95% CI 58.8 to 76.7)) condition compared with the STAND-SIT (52.7 (95% CI 43.8 to 61.5); p<0.001) condition. Significantly higher scores were observed for all four subscales of fatigue during the SIT condition relative to the STAND-SIT condition, indicating greater concentration problems (p<0.001), higher degree of fatigue (p=0.03), reduced motivation (p=0.001) and decreased levels of physical activity (p=0.007).

{kind=link}
Subjective measure of total fatigue (total CIS20-R score) and subscales of fatigue during the SIT (black columns; n=22) and STAND-SIT (white columns; n=23) conditions using the CIS20-R Questionnaire. Data presented as marginal mean (95% CI) adjusted for order of experimental conditions. All measures significantly differ between SIT and STAND-SIT conditions (all p<0.007).
An index of global fatigue (MAF-GFI) did not differ significantly between conditions (STAND-SIT: 13.0 (95% CI 9.1 to 17.0) vs SIT: 15.8 (95% CI 11.6 to 19.9); p=0.47).
Differences in self-reported musculoskeletal symptoms
During the preceding 12 months, a proportion of participants (14 out of 23) reported that they had experienced musculoskeletal symptoms (ache, pain, discomfort) in several anatomical areas; the most common areas being the neck and lower back region (data not shown). As shown in table 1, participants reported significantly fewer musculoskeletal symptoms (ache, pain, discomfort) in the lower back region (32% reduction; p=0.03) and a tendency for fewer symptoms in the ankles/feet (p=0.08) during the STAND-SIT condition compared with the SIT condition. For all other anatomical areas, musculoskeletal symptoms remained consistent between experimental conditions (all p>0.16). For both experimental conditions, participants did not report that their musculoskeletal symptoms in the past 5 workdays prevented them from performing their work tasks (data not shown).
Subjective recall of musculoskeletal discomfort in anatomical regions during the past 5 days of each experimental condition (expressed as a %) according to a modified version of the Standardised Nordic Questionnaire
Differences in self-reported work productivity
Table 2 presents measures of work productivity based on the HWQ. With the exception of work satisfaction (p=0.29), and total HWQ score (p=0.93), which did not differ between conditions, there were trends towards improved overall productivity (p=0.053) and reduced impatience/irritability (p=0.08) in favour of the STAND-SIT condition. Only self-perceived concentration/focus was significantly greater (by 46%) during the SIT condition (p=0.006) compared with the STAND-SIT condition.
Self-reported measures of work productivity based on the Health and Work Questionnaire (HWQ) during the experimental conditions
Acceptability of height-adjustable workstation
As indicated by a higher VAS score, the electric height-adjustable workstation was found to be significantly more enjoyable to use during the STAND-SIT condition (81.0 (95% CI 72.6 to 89.4)) relative to the SIT condition (64.3 (55.5, 73.1); p=0.002).
Discussion
This is the first study to examine, under controlled laboratory conditions, the impact of reducing daily workplace sedentary time by 50% using an electric, height-adjustable workstation on self-reported measures of fatigue, musculoskeletal discomfort and work productivity. We found transitioning from a seated to a standing work posture every 30 min across the workday led to a significant reduction in fatigue levels and lower back discomfort in office workers while maintaining their level of productivity compared with sitting at work only.
The study builds on our previously published work in this specific cohort of adults, showing intermittent standing bouts across the work day reduce cardiometabolic risk, specifically postprandial glucose concentrations.17 Our findings also complement previous ergonomic studies that show the short-term use of height-adjustable workstations by computer workers can help to reduce musculoskeletal discomfort16; our study has, as well, added to the emerging evidence base that shows alternating between a sit/stand work posture can benefit worker productivity and fatigue.13 ,15 ,16
Several recent interventions have focused on the feasibility of height-adjustable workstations to reduce overall sitting time but none have assessed the concomitant impact on workers’ fatigue. We observed an improvement in all aspects of fatigue (including overall fatigue) when replacing 4 h of occupational sitting with standing each workday. These results support the promotion of regular standing breaks across the workday to not only delay the onset of fatigue but to promote concentration, alertness, motivation and activity at work. One potential explanation for the observed improvement in all aspects of psychological fatigue (as assessed by questionnaire) during the STAND-SIT condition is that frequent alternating between postures (sitting and standing) helped reduce muscle fatigue. Psychological fatigue can manifest as a result of muscle fatigue25 and exposure to prolonged sitting at work, which causes low-level static muscle loading (particularly in the lower back, neck and shoulder regions), can promote muscle fatigue via sustained activation of low threshold motor units.26
The level of fatigue experienced by participants while alternating between a standing and seated posture every 30 min was found to be similar to levels reported for healthy office workers (mean±SD score 47.3±19.8).19 Interestingly, the magnitude of the elevated fatigue levels observed in our participants during the sitting only condition was comparable to what has been observed in employees with a somatic reason for fatigue (i.e. recent back operation, pregnant).19
Despite the observed benefit of alternating between a sit/stand work posture on self-perceived fatigue, it was not shown to translate into significantly improved productivity. There was, however, a notable trend towards greater overall productivity (p=0.053) and improved impatience/irritability (p=0.08) in favour of the STAND-SIT condition. Alternating between a sit/stand work posture every 30 min at the very least maintained (i.e. had a neutral effect) workers’ productivity levels, which is consistent with other ergonomic studies.27 Interestingly, our participants reported a reduction in concentration/focus (as measured by the HWQ) when using the height-adjustable workstation to transition between work postures; this finding is in contrast with our other measure of concentration derived from the CIS20-R Questionnaire. It is possible that the need to transition in exact periods of 30 min may have provided an element of distraction for participants while undertaking their work tasks. Participants may have also found it difficult to concentrate/focus on certain work tasks while standing due to a decline in cerebral perfusion (blood flow to the brain). When transitioning from a seated to a standing posture, gravity shifts blood from the thoracic compartment to the lower extremities to cause cerebral hypoperfusion (low blood flow to brain), which is quickly restored through the activation of the baroreceptor reflex.28 It is possible that pooling of blood in the legs and splanchnic circulation during each 30 min standing bout may have reduced cerebral perfusion, impairing participants’ ability to perform some mental tasks.29 ,30
Within the ergonomics literature, it is well documented that musculoskeletal discomfort is most prevalent among adults who either sit14 ,31 or stand32 for prolonged periods at work. In the present study, workers’ reported a significant improvement in lower back symptoms when alternating for 5 workdays between a sit/stand work posture compared with sitting all day. In office workers, the highest prevalence of symptoms is often reported in the spinal area33 as a result of a prolonged sitting posture slackening abdominal muscles to cause curvature of the spine, reducing the flow of synovial fluid to lubricate and nourish the intervertebral discs34 and compressing venous flow in thigh/hip areas.35 ,36 It is possible that alternating postures every 30 min may have enhanced the flow of synovial fluid to the lower back as well as provided a balanced load to the participant's body parts across the day, delaying the onset of any specific musculoskeletal discomfort.
Our study found that participants enjoyed using the height-adjustable workstation to transition between a sit/stand posture significantly more than when the workstation was in a fixed seated position. This is a small but important finding, as such workstations are unlikely to be adopted in workplaces to reduce sedentary time if they are not well accepted.
A major strength of the study was that it was conducted as a randomised, controlled trial under supervised laboratory conditions, which meant we were able to manipulate workers’ sit/stand balance to achieve a 50% reduction in workplace sitting time. Even with organisational support and individual-level behavioural coaching, previous workplace interventions have not been able to achieve a reduction in sitting time of this magnitude.10 A recent field-based non-randomised study by Buckley et al37 examined the acute (1-day) effect of reducing afternoon occupational sitting (13:30–17:30) time with a single bout of standing on continuous glucose measures. While the quantity of occupational sitting time replaced with standing was comparable with the current study, participants were required to stand continuously during the 4 h period as opposed to alternating between work postures. Furthermore, it is not clear what duration of seated work was performed (if any) prior to the single bout of standing.
As reported, we had excellent protocol compliance during the STAND-SIT condition with workers spending on average 50.4% standing and 48.3% sitting during the 8 h workday. An earlier field study looking at the impact of height-adjustable workstations on musculoskeletal discomfort similarly instructed 30 bank tellers to alternate between a sit/stand posture every 30 min across their 7–8 h workday and found the average maximum duration was less than 7 min for sitting and standing bouts.38 We also conducted the study over 5 consecutive workdays; most ergonomics studies examining the effect of altering between a sit/stand posture on productivity, fatigue and musculoskeletal health have only done so acutely (i.e. 42–150 min duration).15 ,16 ,27
A notable limitation of the study was that all outcome measures were self-assessed by participants who were cognisant of the order of experimental conditions (control vs intervention) and it is possible that participants’ prior expectations about the now widely publicised health implications associated with prolonged sitting may have biased their responses in favour of the STAND-SIT condition. While the design of the study precluded participants and research staff from being blinded to the order of conditions, to minimise bias, it would have been preferable to include objective measures of work productivity (i.e. computer-based work task) and musculoskeletal exposure (i.e. electromyography) performed by a blinded third party to support our findings. The restriction of the study to overweight/obese office workers, while necessary to minimise potential confounding influences on the primary outcomes, does limit the generalisability of our findings to the broader working population. Understanding whether the observed benefits of alternating between a seated and standing work posture every 30 min on perceived fatigue and lower back musculoskeletal discomfort can also be identified in healthy, non-obese workers should be the focus of subsequent research.
Future studies are also needed to confirm the efficacy of our intervention in diverse ‘real-world’ settings. This rigorously controlled trial allowed us to assess potential causal links between the promotion of regular standing breaks across the workday and improved indices of worker well-being. However, it is unclear whether achieving a 50% reduction in daily workplace sitting time is feasible outside the confines of the laboratory setting. Previous randomised controlled trials (field-based) in which workers have used height-adjustable workstations at their own discretion to reduce sitting time would suggest that only modest reductions (up to 33 min/workday)7 ,10 are achievable for most workers. Furthermore, removal of the workstations from the office setting results in workers reverting back to their previous habitual sitting patterns.8 With guidelines on how best to reduce sitting time in the workplace for health continuing to remain general and tentative, it is hoped that the current study will help to inform future workplace initiatives and interventions.
Conclusion
The workplace has been identified as a key setting for accumulating prolonged and unbroken sitting time, with office workers being one of the most vulnerable occupational groups. In this laboratory-based trial, we have demonstrated that introducing routine 30 min standing breaks across the workday can reduce workers’ fatigue and lower back discomfort while maintaining levels of work productivity. Based on these findings, workplace initiatives promoting a reduction in workplace sedentary time for health may wish to consider introducing height-adjustable workstations as they are likely to be well accepted and not impact detrimentally on worker behaviour.
Acknowledgments
The authors would like to thank the participants for their involvement, Parneet Sethi for her assistance with the statistical analyses and Louise Hammond for her role as the study's research nurse.
References
Footnotes
-
Contributors AAT, BAK, NO and DWD contributed to the conception and design of research. AAT lead the intervention, collected the data and prepared the manuscript, tables and figures. BAK, NO and DWD reviewed and edited the manuscript. All authors approved the final version of the manuscript.
-
Funding The study was funded by a National Heart Foundation Grant-in Aid (G 10M 5129).
-
Competing interests AAT was supported by a National Heart Foundation of Australia (PH 10M 5413) Postdoctoral Fellowship (Public Health). BAK is supported by a National Health and Medical Research Council of Australia Program Grant (NHMRC #1036352) and a Senior Principal Research Fellowship (NHMRC #1059454). DWD is supported by an Australian Research Council Future Fellowship (FT100100918). NO is supported by National Health and Medical Research Council of Australia Program Grant (NHMRC # 569940) and a Senior Principal Research Fellowship (NHMRC#1003960). All authors are supported by the Victorian Government's Operational Infrastructure Support scheme.
-
Patient consent Obtained.
-
Ethics approval Alfred Hospital Human Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.