Article Text

Extract
Background The comparative effectiveness of non-pharmacological treatments of depression remains unclear.
Methods We conducted an overview of systematic reviews to identify randomised controlled trials (RCTs) that compared the efficacy and adverse effects of non-pharmacological treatments of depression. We searched multiple electronic databases through February 2016 without language restrictions. Pairs of reviewers determined eligibility, extracted data and assessed risk of bias. Meta-analyses were conducted when appropriate.
Result We included 367 RCTs enrolling ∼20 000 patients treated with 11 treatments leading to 17 unique head-to-head comparisons. Cognitive behavioural therapy, naturopathic therapy, biological interventions and physical activity interventions reduced depression severity as measured using standardised scales. However, the relative efficacy among these non-pharmacological interventions was lacking. The effect of these interventions on clinical response and remission was unclear. Adverse events were lower than antidepressants.
Limitation The quality of evidence was low to moderate due to inconsistency and unclear or high risk of bias, limiting our confidence in findings.
Conclusions Non-pharmacological therapies of depression reduce depression symptoms and should be considered along with antidepressant therapy for the treatment of mild-to-severe depression. A shared decision-making approach is needed to choose between non-pharmacological therapies based on values, preferences, clinical and social context.
Statistics from Altmetric.com
Introduction
Depression is one of the most common chronic illnesses and debilitating mental disorders in the USA. Major depressive disorder has a lifetime prevalence of 17% and a 1-year prevalence of 10%. The annual incidence of major depressive disorder is 3%, and rates of recurrence of this condition are high.1 ,2 Depression is a leading cause of significant disability, negatively impacts the quality of life and increases the risk of suicide.3 ,4 The costs and healthcare utilisation of depression are staggering, with an annual overall economic burden estimated to have exceeded 80 billion dollars in the USA in 2000.5 ,6
Multiple antidepressants are available, with selective serotonin reuptake inhibitors being the most widely used. However, there is increasing concern that the efficacy of antidepressants has been overestimated in clinical trials due to unblinding of drug treatments by adverse events.7 Reports of industry bias also fuel debate and concern among patients and healthcare providers about the benefit and harms of antidepressants.8 A meta-analysis has suggested that in mild or moderate depression, improvement with antidepressants may be minimal or non-existent.9 Another meta-analysis suggested that the relationship between initial severity and antidepressant efficacy is attributable to decreased responsiveness to placebo among very severely depressed patients, rather than to increased responsiveness to medication.10
Concerns about antidepressants' efficacy and tolerability in patients with major depressive disorder have led to investigating newer agents with alternative mechanism of action, such as agents that enhance neuroplasticity and neurogenesis.11 These concerns have also led to increased interest in non-pharmacological treatments for depression.
Several non-pharmacological treatments for depression exist, such as cognitive behavioural therapy, naturopathic interventions, psychotherapy and exercise-based interventions. Studies suggest that these interventions may have a beneficial effect on relapse rates following treatment,12 which is critical considering the relapsing nature of depression.
The goal of this study is to summarise the best available evidence about the comparative effectiveness of the various non-pharmacological interventions available for the treatment of depression. We aim to appraise the evidence to facilitate shared decision-making and produce an evidence map that highlights knowledge gaps in the field and aid in developing future research agenda.
Methods
Study design
Owing to the large number of interventions and the availability of published systematic reviews, we conducted an umbrella systematic review (ie, an overview of systematic review; or a systematic review of systematic reviews) (JPT Higgins, S Green. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. http://www.cochrane-handbook.org) and identified eligible randomised controlled trials (RCTs) comparing non-pharmacological treatment options with any other treatment or usual care in patients with depression. We followed a predefined protocol and reported the methodology and findings in accordance with the PRISMA Statement (Preferred Reporting Items for Systematic Reviews and Meta-Analyses).13
Data sources and search strategy
We performed, with no language or time restriction, a comprehensive literature search for systematic reviews published through February 2016 in Ovid (MEDLINE, EMBASE and PsycINFO and the Cochrane Database of Systematic Reviews) and Scopus. The search strategy was developed and executed by an expert reference librarian and two study investigators with experience in systematic reviews. We also reviewed references cited in the American Psychiatric Association guideline on the treatment of major depressive disorder14 and sought additional references from content experts. The detailed search strategy is provided in the online supplementary appendix.
Supplementary appendix
Eligibility criteria
We included any systematic review of RCTs that (1) enrolled adults (aged ≥18 years) with a diagnosis of unipolar depression; (2) compared a non-pharmacological treatment with another non-pharmacological treatment, a pharmacological treatment or usual care; and (3) included at least one outcome of interest (table 1). The included interventions were reviewed by a clinical expert and grouped into 11 intervention groups (table 2). The outcomes of interest were the efficacy and effectiveness of the intervention (depression symptoms and severity), adverse events and dropout rate (withdrawal from the study and inability to continue the intervention for any reason). Outcomes are defined in online supplementary appendix table 1.
The question of this systematic review (comparative effectiveness of treatments for depression)
Types of interventions evaluated in this review
Study selection
Pairs of reviewers (WHF, MA, MM, FA, MHF, ATA, JA, EAM, MRG, AC-G, KM, NA) working independently identified eligible systematic reviews by screening titles, abstracts and then full texts. Disagreements were resolved by consensus or arbitrated by a third reviewer (MHM, AL), if necessary. We assessed chance-adjusted agreement (κ statistic) for each step requiring judgement.
We chose a single systematic review for each comparison and outcome. We based this choice on (1) the credibility15 of the process of the systematic review (ie, chose the most rigorous review), (2) comprehensiveness of the search of the review (ie, chose the most inclusive review with the largest number of included RCTs) and (3) date of conducting the systematic review (ie, chose the most recent).
Data extraction
Pairs of reviewers (WHF, MA, MM, FA, MHF, ATA, JA, EAM, MRG, AC-G, KM, NA) extracted data using a standardised, piloted, online form. We extracted data on patient characteristics, severity of depression, type of interventions and depression scales used to assess outcomes.
The outcomes of this study were assessed as either dichotomous variables (the proportion of patients who report improvement of depression symptoms, dropout, report side effect, achieve remission, or relapse) or as continuous variables (depression severity scales). For dichotomous outcomes, we extracted the number of patients with the outcome and the total number of patients at risk. For continuous outcomes, we extracted the mean, SD and sample size.
Risk of bias assessment and quality of evidence
Methodological quality of the systematic reviews was assessed using the AMSTAR instrument (a measurement tool to assess the methodological quality of systematic reviews).16 The Cochrane Collaboration risk-of-bias tool was used to evaluate the risk of bias of the included RCTs (JPT Higgins, The Cochrane Collaboration, 2011). Pairs of reviewers (WHF, MA, MM, FA, MHF, ATA, JA, EAM, MRG, AC-G, KM, NA) working independently assessed the risk of bias for random-sequence generation; allocation concealment; blinding of patients, caregivers or outcome assessors; incomplete outcome data; selective reporting; and other biases (funding source and nature). Disagreements were resolved by discussion or arbitrated by a third reviewer (AL, MHM). We summarised the risk of bias for all domains to produce an overall risk of bias for every trial (JPT Higgins, The Cochrane Collaboration, 2011). The risk of bias was considered to be high if there was a concern for bias in any key domain (allocation concealment or blinding of patients), low if the risk of bias was low for all key domains, and unclear in all other cases. We chose a priori to consider allocation concealment and blinding as key quality domains because of their relative importance for preventing selection bias and bias in the assessment of subjective outcomes, such as depression scales.
The quality of evidence (ie, certainty in the evidence) was evaluated using the GRADE approach (Grading of Recommendations, Assessment, Development and Evaluation).17 We constructed an evidence map, which is a visual depiction of the characteristics of evidence in a particular field.18 This map illustrates the quality and the quantity of evidence based on a systematic search (ie, which interventions were compared head-to-head and how trustworthy were such comparisons) and can aid in demonstrating gaps in knowledge and future research needs of a broad field.18
Data synthesis and analysis
For continuous outcomes (ie, depression severity measured using a scale), we estimated the effect of interventions using the standardised mean difference. In this approach, measurements on different scales are standardised (reproduced in SD unit) to allow pooling in meta-analysis. For dichotomous outcomes, we estimated the relative risk. We constructed the D–L random effects models to pool estimates of effects across trials. We were not able to conduct network meta-analysis to combine direct and indirect evidence of class and agent comparisons due to substantial heterogeneity across trials.
We used the I2 statistic and the Q statistic to assess heterogeneity. I2 >50% and/or the p value for Q test <0.10 suggests substantial heterogeneity. Evaluation for publication bias was not possible because of large heterogeneity that makes statistical tests for funnel plot symmetry unreliable.19 Statistical analyses were conducted using a specialised statistical package (StataCorp. 2015. Stata Statistical Software: Release V.14. College Station, Texas: StataCorp LP).
Result
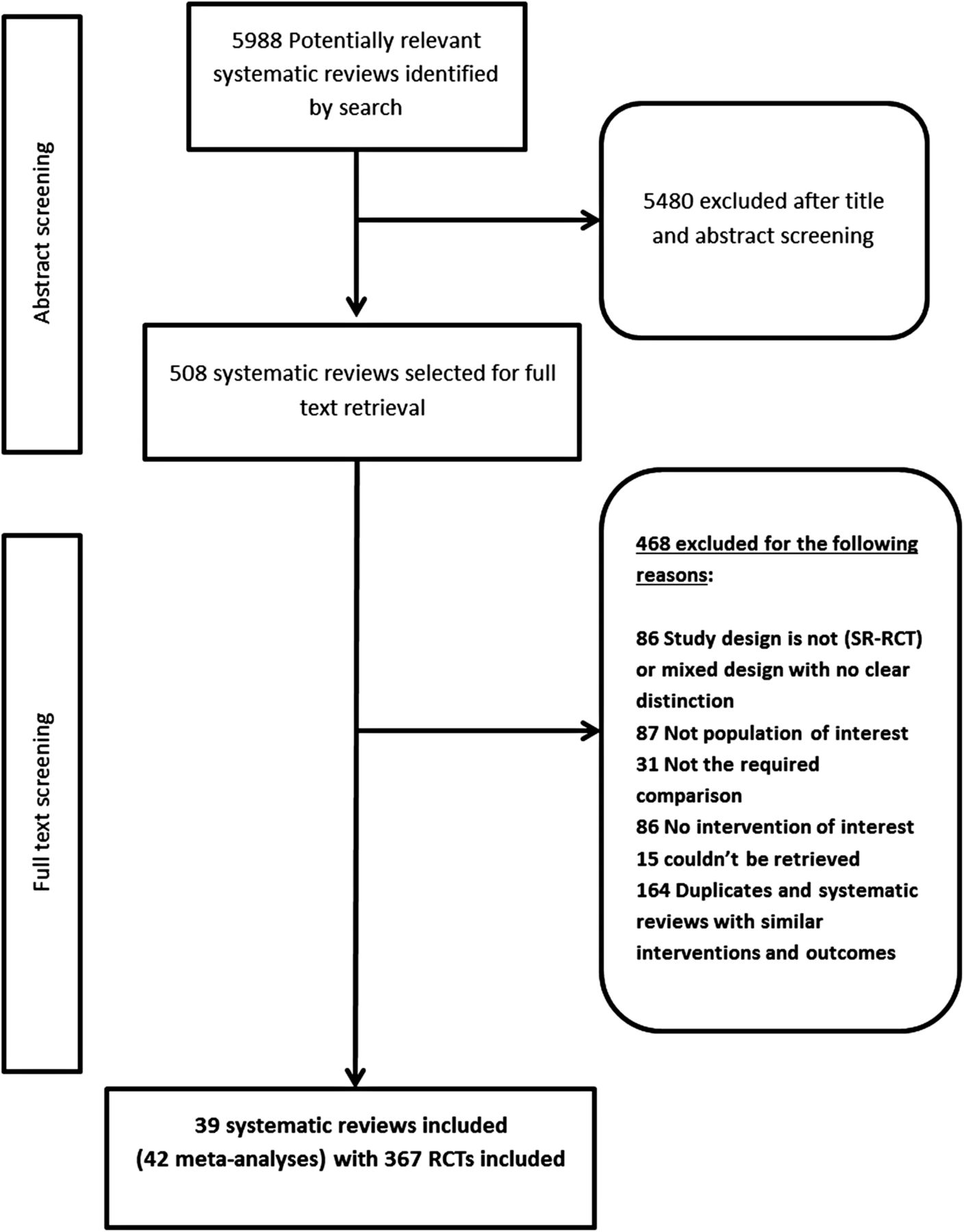
The electronic search yielded 5988 potentially relevant citations; of which 39 systematic reviews20–54 were used to identify 367 primary RCTs enrolling ∼20 000 patients for a total of 11 different treatment options and 17 unique head-to-head comparisons (figure 1). The systematic reviews are described in online supplementary appendix table 2. The most commonly studied interventions were antidepressants, cognitive behavioural therapy, biological interventions (electroconvulsive therapy, transcranial direct current stimulation and transcranial magnetic stimulation), naturopathic interventions (herbs, supplements and acupuncture) and psychotherapy.

Summary of study selection process.
Outcomes
Severity of depression
Three hundred and five RCTs (∼20 000 participants) were identified in 33 systematic reviews reporting on the efficacy of different treatment options using standardised depression scales, with 17 unique head-to-head comparisons with moderate-to-low certainty evidence.
Comparison with the control group (waitlist, usual care or placebo)
Each of CBT (61 RCTs), computerised cognitive behavioural therapy (14 RCTs), naturopathic therapy (43 RCTs), biological interventions (12 RCTs) and physical activity interventions (61 RCTs) reduced depression severity compared with a control group (waitlist, usual care or placebo). Forest plots are presented in online supplementary appendix figures 1–5.
Comparison with other interventions
Cognitive behavioural therapy reduced depression severity compared with antidepressants (9 RCTs), interpersonal therapy (7 RCTs) and psychotherapy (12 RCTs). No significant difference was reported when cognitive behavioural therapy was compared with psychodynamic therapy (7 RCTs) or acceptance therapy (2 RCTs). Naturopathic therapy (40 RCTs) and biological interventions (7 RCTs) were each associated with a reduction in depression symptoms compared with antidepressants. There was no significant difference when physical activity interventions were compared with AD (5 RCTs). There was no significant difference between psychotherapy and antidepressants. There was no significant difference between interpersonal therapy and antidepressants (2 RCTs). Forest plots are presented in online supplementary appendix figures 1–8.
Remission
Sixty-nine RCTs (7455 participants) retrieved from seven systematic reviews reported on remission rate, with seven unique comparisons with moderate-to-low certainty evidence.
Comparison with the control group (waitlist, usual care or placebo)
Meta-analysis showed no significant difference in remission rate between cognitive behavioural therapy and no treatment (7 RCTs). Biological (16 RCTs) and naturopathic (12 RCTs) interventions improved remission compared with no treatment; however, the certainty in this evidence was low. Forest plots are presented in online supplementary appendix figures 9–11.
Comparison with other interventions
Meta-analysis showed no significant difference in remission rate between cognitive behavioural therapy and antidepressants, interpersonal therapy or psychotherapy (see online supplementary appendix figure 8). Meta-analysis showed no significant difference in remission rate between naturopathic interventions compared with antidepressants (12 RCTs) (see online supplementary appendix figure 11).
Clinical response
One hundred and thirty-eight RCTs (13 388 participants) reported clinical response as an outcome, evaluating 10 unique comparisons with moderate-to-low certainty evidence.
Comparison with the control group (waitlist, usual care, placebo)
When compared with a control intervention, cognitive behavioural therapy (9 RCTs), naturopathic therapy (38 RCTs), biological interventions and psychotherapy all increased the likelihood of achieving clinical response. Forest plots are presented in online supplementary appendix figures 12–15.
Comparison with other interventions
There was no significant difference between cognitive behavioural therapy and acceptance therapy, antidepressants, interpersonal therapy, psychodynamic therapy or psychotherapy (33 RCTs, 2835 participants). There was no significant difference in response rate between naturopathic therapy and antidepressants. Forest plots are presented in online supplementary appendix figures 12 and 13.
Dropout rate
One hundred and thirty-three RCTs (12 446 participants) retrieved from 8 systematic reviews reported on the rate of dropout from treatment (for any reason), including 12 unique comparisons with overall moderate-to-low certainty of evidence.
Most analyses of this outcome were not statistically significant, suggesting similar dropout rate between antidepressants, acceptance therapy, interpersonal therapy, psychodynamic therapy, psychotherapy, physical activity interventions, biological interventions or control interventions (107 RCTs, 5679 participants) (see online supplementary appendix figures 16–19). Naturopathic therapy and cognitive behavioural therapy were associated with lower and higher dropout rates, respectively, when compared with antidepressants (see online supplementary appendix figures 16 and 19).
Relapse rate
One systematic review (6 RCTs and 241 participants) showed that antidepressants use was associated with higher relapse rate compared with cognitive behavioural therapy (see online supplementary appendix figure 20). Data on other non-pharmacological therapies were sparse.
Side effects
Antidepressant use was associated with higher rate of side effects than naturopathic interventions or placebo (see online supplementar appendix figure 21).
Evidence map
An evidence map for efficacy and adverse effects is depicted in figure 2. The map highlights the paucity of most pairwise head-to-head comparisons. The majority of comparisons were against a control group of no treatment or usual care. The description of usual care is usually not well reported in the literature, making the available evidence less helpful for comparative effectiveness inferences. In addition, the map shows that the quality of evidence was low in most of the comparisons.

{kind=link}
{kind=link}
Evidence map: availability and quality of the evidence. RCT, randomised controlled trial. Blue area represents the evidence of harms and side effects; grey area represents the evidence of treatment benefits. Quality of evidence: green (high), yellow (moderate), red (low) and empty cells (no evidence). *Depression scale, **clinical response, ***remission, ****reduction in depression scale. †Dropout rate, †† side effects, ††† relapse rate.
Discussion
Clinical implications
This systematic review demonstrates that non-pharmacological therapies can reduce depression severity as measured using standardised scales. The relative efficacy among the various non-pharmacological therapies on depression severity is however lacking. In terms of remission and relapse rate, data were sparse. As expected, side effects of non-pharmacological therapies were lower than those reported with antidepressants. Dropout rates (ie, discontinuing treatment for any reason) were similar to antidepressants.
Considering the plausible benefit-to-harm ratio of non-pharmacological therapies, these therapies can be recommended to patients based on the clinical context and patients' values and preferences. For example, subclinical to moderate severity depression, recent onset or shorter duration episodes may benefit from these interventions as a monotherapy. Severe depression may be better treated with antidepressants as an initial therapy. Prior good response to non-pharmacological therapy is an indicator for using the same therapy. Patients with significant functional impairment and low energy would not be candidates for cognitive behavioural therapy because it requires actual effort and engagement from the patient. Patients and clinicians concerned about the regulation of supplements and biological treatments would not opt for such treatment (eg, supplements are not regulated in the USA by the Federal Food and Drug Administration). Non-pharmacological treatments in general are tightly controlled in randomised trials; however, in practice, providers may have variable training and expertise. Therefore, the fidelity to such treatments is difficult to ascertain. Consequently, recommendation of non-pharmacological therapy should be made after considering the availability and feasibility of good quality provider in the patient locale. Patients, who are particularly averse to drugs and worry about side effects, may prefer a natural or non-pharmacological therapy. Finally, severe, relapsing and chronic cases of depression can benefit from step-up therapy with aggressive combination of antidepressants and psychotherapy or intense cognitive behavioural therapy.55
Since several non-pharmacological interventions appear to have similar effectiveness. Shared decision-making is needed to engage patients and their families to make informed choices about which treatment approach is most consistent with their values and preferences. Tools are also needed to facilitate shared decision-making and make it operational (ie, decision aids).
Limitations and strengths
We followed an umbrella systematic review approach (ie, identified randomised trials from published systematic reviews). This approach has inherent limitations and is restricted to the quality of reporting and rigour of existing systematic reviews. The evidence has clear limitations that relate to the small number of head-to-head comparisons and heterogeneity of interventions, patients, measurement scales and follow-up length across studies. Seven of the systematic reviews reported high likelihood of publication bias. Non-pharmacological interventions are considered complex multicomponent interventions.56 The current literature does not report well the characteristics of such interventions (who delivered the intervention, level of expertise, location, duration, frequency and intensity of the intervention, etc). All these characteristic are likely covariates that affect the effectiveness observed in trials of complex interventions. Better reporting of such characteristic would allow evaluating the role of the various components and facilitate replication of the intervention and translation from research setting into practice. This review focused on adults with depression, which makes the result not applicable to children and pregnant women. The strengths of this review include the comprehensive literature search across multiple databases and the duplicate process of selecting and appraising studies.
Research implications
The available trials had short-term follow-up, focused exclusively on relief of depressive symptoms, and had substantial potential for the risk of bias. Longerterm trials focusing on sustainability of beneficial effects, functional status and health-related quality-of-life outcomes are needed. Review of the evidence map shows that head-to-head pragmatic trials are needed (as opposed to comparisons against placebo interventions in tightly controlled research setting). Such pragmatic comparative effectiveness trials would provide patients, clinicians and decision makers with more useful evidence. The map also shows the need for more trustworthy evidence (ie, trials with bias protection measures, particularly allocation concealment). The National Academy of Medicine (formerly called the Institute of Medicine) has listed the comparative effectiveness of different depression treatments as one of their 100 initial priority topics for comparative effectiveness research.57
Conclusion
Non-pharmacological therapies of depression reduce depression symptoms and should be considered along with antidepressant therapy for the treatment of mild-to-severe depression. A shared decision-making approach is needed to choose between non-pharmacological therapies based on values, preferences, clinical and social context.
References
Footnotes
Contributors WHF screened literature, data extraction of the identified studies, carried out data cleaning and statistical analysis and drafted the manuscript. MA, MM and FA screened and data extraction of the identified studies, carried out data cleaning and approved the final version of the manuscript. MHF, ATA, EAM, JA, MRG, AC-G, KM and NA screened and data extraction of the identified studies and approved the final version of the manuscript. CNS and MDW contributed to clinical expertise to the project and approved the final version. ZW approved the final version of the manuscript and contributed a methodological expertise. LJP approved the final version of the manuscript and designed the search strategy. MHM and AL conceived the idea, wrote the protocol, contributed the methodological expertise and approved the final version of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
▸ Additional material is published online. To view please visit the journal (http://dx.doi.org/10.1136/ebmed-2016-110522).