Article Text

Abstract
Objectives: To determine the long term survival and predictors of death in patients with primary intracerebral haemorrhage (ICH) in Central Finland.
Methods: Data were collected retrospectively on all adult patients with first ever ICH in Central Finland county between September 1985 and December 1991. The survival of all patients at the end of December 2002 was investigated. Kaplan–Meier survival curves were constructed and factors associated with both early (⩽28 days) and late deaths determined. Long term survival was compared with the general Finnish population of the same age and sex distribution. The causes of death were compared with those of the population of Central Finland.
Results: 411 patients with first ever ICH were identified, 199 men (mean age 64.9 years) and 212 women (mean age 69.5); 30 died before hospital admission, and 208 (50.6%) within the first 28 days. In Kaplan–Meier analysis, at 16 years the cumulative survival was 3.2% for men and 9.8% for women. The 28 day survivors had a 4.5-fold increased annual risk of dying during the first year after ICH, and 2.2-fold during years 2 to 6. On admission, significant independent predictors of death within the first four weeks were unconsciousness, lateral shift of cerebral midline structures, mean arterial pressure ⩾134 mm Hg, hyperglycaemia, anticoagulant treatment, and ventricular extrasystoles. Predictors of late death for the 28 day survivors were old age, male sex, and heart failure.
Conclusions: Primary intracerebral haemorrhage has a poor short and long term outcome. The results emphasise the importance of primary and secondary prevention for ICH.
- ICH, intracerebral haemorrhage
- MAP, mean arterial blood pressure
- primary intracerebral haemorrhage
- predictor
- long term survival
Statistics from Altmetric.com
The short term survival of primary intracerebral haemorrhage (ICH) has been documented in several reports. During the first month after ICH onset the proportion dying has varied from 22% to 62%.1,2 Studies on long term survival are few: in six the follow up has been for five years or longer,2–7 and in only three studies has the follow up been for 10 years or more.2,5,7
The present analysis of epidemiologically representative ICH patient material was made in order to improve our knowledge of the long term survival and its determinants. We also compared the survival with the age and sex matched general population, and the distribution of the causes of death with that of the basic population from which the patients emerged.
METHODS
We collected data retrospectively on all adult patients who suffered from ICH between September 1985 and December 1991 in a population of 249 500 (1988) living in the catchment area of the Central Hospital of Central Finland (the county of Central Finland). The patients were traced from the discharge lists of the two hospitals and 18 health centres in the area, from death certificates, and from the medical and medicolegal necropsy reports. A prerequisite for accepting ICH as the cause of stroke was confirmation by cranial computed tomography (CT) or necropsy. Secondary ICHs caused by trauma, arteriovenous malformations, or rupture of arterial aneurysms were excluded. In all, 411 patients with first ever ICH were traced, 381 of whom were admitted to the Central Hospital.
The vital status of all patients was checked at the end of December 2002. All medical records held by the Central Hospital, Jokilaakso Hospital, and the health centres were reviewed for recurrent strokes and survival. If necessary, the death certificates were retrieved. The causes of death were classified in five broad groups:
-
Vascular diseases included deaths from first ICH, recurrent ICH, new ischaemic or non-specified stroke, coronary heart disease and other cardiac causes, pulmonary embolism, and other vascular causes;
-
pneumonia, whether or not associated with first or recurrent ICH;
-
malignant diseases;
-
traumatic causes;
-
miscellaneous diseases.
The information about earlier diseases and current anticoagulant use obtained from the patients or relatives was confirmed by reviewing the previous medical records. Diabetes was recorded in patients on insulin, oral hypoglycaemic drugs, or on dietary restriction, and hypertension if antihypertensive drug treatment was being prescribed. Smoking habits were categorised as never or ever smokers.
Blood pressure was measured on admission, in 94% within 48 hours after stroke onset. Mean arterial pressure (MAP) was calculated by adding one third of the pulse pressure (systolic minus diastolic blood pressure) to the diastolic pressure. The level of admission consciousness was graded as 1, conscious (alert, somnolent, disoriented); and 2, unconscious/comatose (depending on the response to painful stimuli).
Blood glucose was measured in 345 patients (91% within 48 hours after stroke onset), and 343 had cranial CT (87% within 48 hours after stroke onset). All CT films were available for analysis, which included measurement of haematoma volume (ml) and lateral shift (mm) of cerebral midline structures, evaluation of intraventricular or subarachnoid spread, and hydrocephalus. Haematoma volume was measured using a planimetric computer program.8
Statistical methods
We used χ2 testing to search for variables that were individually associated (p<0.1) with the short term (⩽28 days) and long term (>28 days) survival. Twenty six variables were included: age (tertiles), sex, presence of hypertension, coronary heart disease including myocardial infarction, heart failure, diabetes, anticoagulant treatment, smoking habits (never/ever smokers), consciousness (conscious/unconscious), MAP and blood glucose (both dichotomised at median), haematoma volume (quartiles), midline shift (tertiles), presence of intraventricular or subarachnoid spread, and hydrocephalus. The following ECG items were included: left ventricular hypertrophy, pathological Q wave, atrial fibrillation, left bundle branch block, tachycardia (heart rate >100 beats/min), bradycardia (heart rate <60 beats/min), ST segment elevation >2.5 mm, ST segment depression >1.0 mm, ventricular extrasystoles, and a negative T wave.
Hemiparesis was not included in the variables because a reliable evaluation in unconscious patients is usually impossible. The large number of patients who died soon after admission before any examinations were done explains the missing data on, for example, cranial CT.
The Kaplan–Meier technique was used to generate survival curves for men and women, and the age tertiles. Logistic regression and Cox proportional hazards regression analyses were undertaken on patients admitted to hospital to identify significant independent predictors of short and long term survival. The analyses were carried out both with and without mean substitution of missing data. Individual variables that were associated (p<0.1) with survival were included in the analyses. All CT variables were highly intercorrelated and we chose—because of easy accessibility—lateral shift of the midline structures to represent the CT findings. Forward Wald stepwise selection with entry 0.05 and removal 0.1 was used. All statistical calculations were done using SPSS software (version 10.0).
The expected survival of the age and sex matched general population was calculated from Finnish Life Tables 1998. The causes of death were compared with the average annual numbers of deaths during a five year period (1994 to 1998) in the population of Central Finland (http://statfin.stat.fi/stat.web/).
The study protocol was approved by the Finnish Ministry of Social Affairs and Health, which authorised the perusal of all case reports of ICH patients who lived in the Central Hospital District.
RESULTS
Between September 1985 and December 1991 we identified 411 first ever ICH patients in the study population (incidence 26/100 000/year): 199 men (mean (SD) age, 64.9 (11.5) years), and 212 women (69.5 (11.1) years). Eighty four per cent of the haematomas were supratentorial and 16% infratentorial. Thirty patients died before admission, and 381 were admitted to the emergency room of the Central Hospital, 91% within 24 hours of ICH onset. There were 359 patients who were treated conservatively, and 26 who had surgical evacuation of the haematoma. The median follow up for individual patients was 26 days (range 0 to 6191 days).
The early case fatality was very high; 91 patients (22%) died within 24 hours of onset, 173 (42%) were dead on day 7, and by four weeks after onset 208 had died (51%, 95% confidence interval (CI), 46% to 55%). At one year, 58% had died (95% CI, 53% to 62%; fig 1), and at five years, 73% (69% to 78%). At 16 years after the ICH the cumulative Kaplan–Meier survival was 6.3% for men, and 9.8% for women. The causes of death of the 208 patients who died during the first 28 days were: the index ICH (200), pulmonary embolism (4), myocardial infarction (3), and mesenteric artery thrombosis (1).
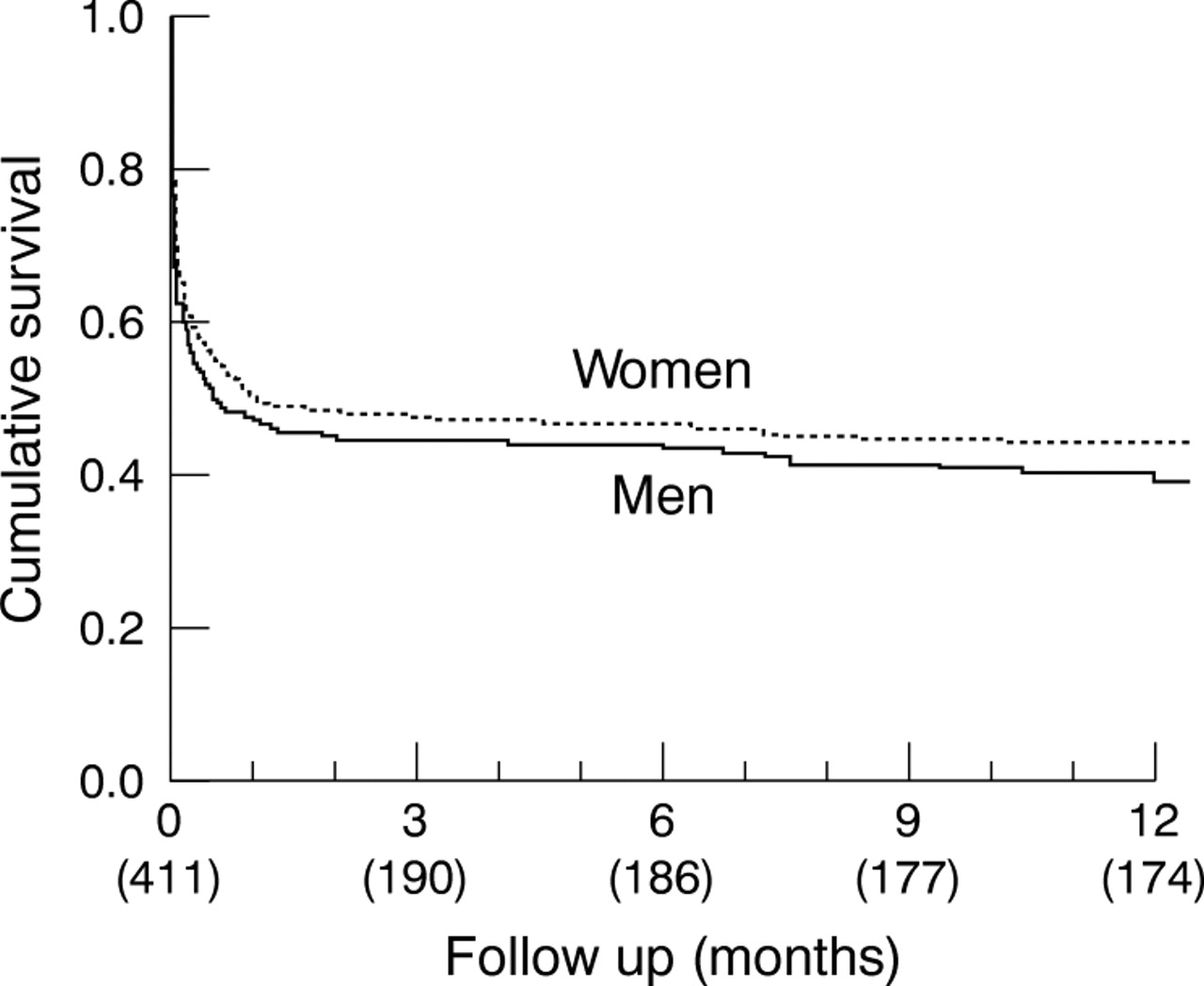
Kaplan–Meier curves showing the probability of 12 month survival, by sex. Numbers of patients in brackets.
Twenty eight day survival
Sixty one (16%) of the 381 patients who were admitted died on the day of admission. In single explanatory variable analysis, 13 variables were associated with death during the first four weeks: unconsciousness, haematoma volume, midline shift, intraventricular and subarachnoid spread, hydrocephalus, anticoagulant treatment, atrial fibrillation, tachycardia (heart rate >100 beats/min), ventricular extrasystoles, negative T wave, blood glucose >7.3 mmol/l, and MAP >134 mm Hg. Logistic regression analysis of 312 patients with complete data revealed six significant independent predictors of death during the first four weeks (table 1). Unconsciousness and lateral shift of cerebral midline structures ⩾6 mm were the most important predictors. The odds ratios of MAP ⩾134 mm Hg, blood glucose ⩾7.7 mmol/l, anticoagulant treatment at the time of ICH onset, and ventricular extrasystoles in the ECG varied from 3.2 to 2.6. Analysis of all 381 admitted patients with mean substitution of missing data gave a similar result.
Significant independent predictors of death during the first 28 days after onset of intracerebral haemorrhage
Owing to missing clinical evaluation, the 30 patients who died before admission were not included in the analysis. The mean age and prevalence of previous diseases were similar to the 381 admitted patients, but the proportion of men was higher (p = 0.012).
Long term survival
Long term survival was analysed on the basis of the 203 patients who were alive after the first 28 days. Single explanatory variables associated with long term survival were old age, male sex, coronary heart disease, heart failure, and atrial fibrillation. In Cox regression analysis, only three variables appeared as significant independent predictors of death during long term follow up. Age over 73 years was the most important, followed by heart failure and male sex (table 2).
Significant independent predictors of late death in the 28 day survivors
Figure 2 shows the Kaplan–Meier survival curves for age tertiles. Patients less than 65 years of age had the best prognosis, with 19.3% surviving for 16 years after ICH; of the two groups of older patients only 2.7% and 1.8% were alive. Compared with the general Finnish population of the same age and sex, the annual risk of dying during the first year was increased 4.5-fold and during years 2 to 6, 2.2-fold; after this the risk declined and was 0.9-fold during years 7 to 16. The patients who died during the first six years were significantly older and had a higher prevalence of hypertension, heart failure, atrial fibrillation, and hydrocephalus than the six year survivors.

{kind=link}
{kind=link}
Kaplan–Meier curves showing the probability of long term survival, by age tertiles. Numbers of patients in brackets. + = censored cases.
As stated above, 200 of 208 deaths within 28 days after onset were from the index ICH. The causes of death of the 159 patients dying after day 28 were quite different, and only 34% were from cerebrovascular disease. However, the distribution of causes of death of the 28 day survivors differed from that of the general population of Central Finland (table 3). The odds ratios of death from cerebrovascular diseases and pneumonia were 4.0 and 3.9, respectively, but only 0.5 for coronary heart and 0.4 for malignant diseases.
Causes of death during the long term follow up of the patients with intracerebral haemorrhage who survived the first 28 days
Recurrent strokes
Seventy one (35%) of the 28 day survivors had recurrent strokes during the follow up. Twenty three patients had verified ICH, two of them twice, and one three times. The first recurrence occurred at a median of 30 months (range 2 to 158) after the index ICH, and 50% of the recurrences were fatal. Twenty one patients suffered from ischaemic stroke at a median of 74 months (range 4 to 168) after ICH, and 27 from an undefined stroke at median 55 months (range 1 to 174) after ICH. Of the ischaemic and undefined strokes, 27 were fatal.
DISCUSSION
The acute case fatality rate of ICH was very high. Every fifth patient died on the day of ICH onset, and 51% were dead by 28 days. The most important independent predictors of death within the first 28 days were unconsciousness on admission and ⩾6 mm lateral shift of cerebral midline structures. Other predictors were high admission MAP and blood glucose, current anticoagulant treatment, and ventricular extrasystoles on the ECG.
The predictors of dying during long term follow up of the 28 day survivors were old age, heart failure, and male sex. During the first year after ICH, the risk of dying among the 28 day survivors was increased over fourfold compared with the general Finnish population of the same age and sex. Thereafter the risk diminished, and after six years there was no difference.
The strengths of the study are the large number of epidemiologically representative patients. Because not all stroke patients in the population had CT, or necropsy in the case of death, some ICH patients must have remained undiagnosed. The annual incidence 26/100 000 obtained in the present study is, however, not significantly smaller than the 31/100 000 obtained in an epidemiological study of 158 patients from a restricted area of Central Finland, the Jyväskylä region, from which virtually all acute strokes were admitted to the Central Hospital.8 These 158 patients are included in the patient material of this study.
The weaknesses of the study mainly reflect its retrospective nature; not all the patients had complete baseline data, the timing and performance of auxiliary examinations varied, and follow up often depended on reviews of the medical records and death certificates.
The 28 day case fatality of 51% (95% CI, 46% to 55%) in our study, which includes patients who died before admission, is similar to the mean value in previous population based studies of 50% (95% CI, 46% to 54%)2,9,10,11,12 but significantly higher than the 39% (37% to 41%) obtained from hospital based studies.1,5,6,13,14,15,16,17,18,19,20 Because there is no effective treatment for ICH, different case mixes probably explain these divergent rates. Age may not be a decisive factor because the mean ages of all these studies has been between 60 and 69 years. Different time lags between ICH onset and admission could, on the other hand, explain the difference fairly well, because late admissions exclude patients dying acutely after ICH onset.
At one year, 58% of our patients had died—similar to the mean of previous population based studies of 59% (95% CI, 54% to 63%)2,3,11 but again significantly higher than the 50% (48% to 53%) in the hospital based studies.5,6,12,19 At five years, the situation was similar, the present study and previous population based studies2–4 being of the same magnitude (73% and 71% deceased, respectively) but only 61% (95% CI, 59% to 64%) were dead in the hospital based studies.5,6 The same trend is obvious in studies with 10 years of follow up. In the Danish study,2 (Brönnum-Hansen H, personal communication), 81% of the patients were dead at 10 years, and 89% at 15 years. In Perth, extrapolated from the Kaplan–Meyer curve, 75% were dead at 10 years.7 The results of the present study, with 82% dead at 10 years and 90% dead at 15 years, are of the same magnitude as the two earlier population based studies. In the only hospital based study from Toronto, the 10 year and 13 year mortalities, extrapolated from the Kaplan–Meier survival curve, were much lower, at 48% and 54%, respectively.5 It is reasonable to assume that the lower mortality from hospital based studies reflects the omission of prehospital deaths.
Independent significant predictors of early death have been identified by multivariate analysis in eight studies.1,5,13,14,16–19 Old age, disturbed consciousness/low Glasgow coma scale score, haematoma volume, intraventricular and subarachnoid spread, midline shift, narrow pulse pressure, high pulse pressure, infratentorial location, and high blood glucose have been such predictors. In our study, in addition to unconsciousness, midline shift, and high blood glucose, an admission MAP of ⩾134 mm Hg, anticoagulant treatment, and ventricular extrasystoles emerged as independent predictors.
Old age has been found to be an exclusive predictor of death during a five year follow up of ICH patients who recovered and returned home after a mean of 29 days from onset (Vermeer S, personal communication).6 There are no comments about other predictors in the few long term follow up studies. We were able to identify three significant independent predictors of death during the long term follow up of the 28 day survivors: old age, cardiac failure, and male sex.
Conclusions
ICH is still a serious disease, with every fifth patient dying within 24 hours of onset, 50% dying by four weeks, and according to Kaplan–Meier analysis, only around 8% being alive after 16 years. We were able to identify six variables that predicted death within the first 28 days after onset, and three predictors of death during long term follow up. Unfortunately, most of the predictors are not amenable to treatment. In theory, a high admission MAP and blood glucose could be treated, but the possible impact of this on the outcome is an open question. In addition, there is no agreement on the value of surgical evacuation of supratentorial haematomas.
Primary and secondary prevention in addition to good care in the acute phase are presently the only means of managing the problem of ICH. The value of long term antihypertensive treatment as primary and secondary prevention is not questioned. The role of active treatment of high blood pressure during the acute phase remains open.
Acknowledgments
We thank Drs Henrik Brönnum-Hansen, Sarah Vermeer, and Michael Hill for providing us with detailed data from their studies.
REFERENCES
Footnotes
-
Competing interests: none declared