


Abstract
Background Obesity is a top-priority global health issue; however, a clear way to address obesity in primary care is not yet in view.
Aim To conduct a meta-ethnography of patient and primary care practitioner perspectives of roles and responsibilities in how to address obesity in the UK, to inform evidence-based services that are acceptable to, and appropriate for, patients and practitioners.
Design and setting Qualitative synthesis applying meta-ethnographic methods according to the Noblit and Hare monograph. Database searches in MEDLINE®, Social Sciences Citation Index®, CINAHL, and Health Management Information Consortium were limited to 1997–2012 to examine recent perspectives.
Method Full articles of practitioner and/or patient perspectives on obesity services in primary care were reviewed, and included semi-structured or unstructured interviews and focus groups, and participant observations.
Results Nine studies were synthesised with perspectives from patients (n = 105) and practitioners (n = 144). Practitioners believe that patients are responsible for obesity, and that primary care should not help, or is poorly equipped to do so. Patients ‘take responsibility’ by ‘blaming’ themselves, but feel that practitioners should demonstrate more leadership. The empowerment of patients to access health services is reliant on the empowerment of practitioners to take an unambiguous position.
Conclusion Primary care has the potential either to perpetuate or counter obesity-related stigma. There needs to be a firm decision as to what role primary care will take in the prevention and treatment of obesity. To remain ambiguous runs the risk of losing patients’ confidence and adding to a growing sense of futility.
- meta-ethnography
- obesity management
- patient perspectives
- practitioner perspectives
- primary care
- qualitative synthesis
INTRODUCTION
Obesity is recognised globally as a top priority by health professionals, policy makers, economists, and the public.1–3 However, a clear way about how to address obesity in primary care is not yet in view. Primary care has increased its preventive services; a position supported by the British Medical Association (BMA).4 Clinical guidance on obesity is based on consensus of evidence from policy and healthcare practitioners,5,6 yet what is delivered in practice varies.7
The recent epidemiological shift from acute to chronic illnesses marked the rise of the ‘lifestyle era’.8 Fatness is now framed as a social irresponsibility, from poor parenting to overburdening health services,9,10 and the common response is to focus on individual responsibility and behaviour change.11,12 Conversely, the landmark Foresight report emphasises wider determinants of obesity (for example, psychosocial, infrastructural, and economic).13 Despite the report’s overwhelming evidence, policy and practice tend to ‘drift’ back to lifestyle approaches.14
Qualitative literature exists on practitioner and patient perspectives on obesity services in primary care; however, a synthesis has not yet been carried out. This study aimed to synthesise patient and primary care practitioner perspectives of roles and responsibilities in how to address obesity in the UK.
METHOD
Literature review
The literature review followed Centre for Reviews and Dissemination guidance.15 PICOS terms were used to conduct keyword searches: ‘primary care’ (Population); ‘obesity services’ (Intervention); ‘perspectives’ (Outcomes); and ‘qualitative’ (Study design). Databases (MEDLINE®, Social Sciences Citation Index®, CINAHL, and Health Management Information Consortium), key academic journals, and bibliographic references were searched.
English language studies published from 1997 to 2012 were included to examine recent perspectives. Only UK-based studies were examined to produce an in-depth understanding of the unique culture and health systems in the UK. Practitioners were those who deliver obesity services in primary care (healthcare and community settings). Patients were of any age. Ethnographic accounts included semi-structured or unstructured interviews and focus groups, and participant observations. Surveys and structured interviews were excluded. The desired final sample was one that provided both breadth (geography, participant, and service) and depth (descriptions of context) of topic. Quality was assessed using the Critical Appraisal Skills Programme method.16
Synthesis
Qualitative methods are able to enhance health policy and practice through understanding people’s beliefs and practices.17–19 This meta-ethnography followed methods according to Noblit and Hare,20 summarised in Figure 1.

Analysis process.
How this fits in
Obesity is a global health issue that has proven a challenge to address in the primary care setting. Qualitative research on patient and practitioner perspectives on obesity-related primary care services has been conducted in the UK, but a synthesis of these perspectives has yet to be conducted. A lack of consensus about who is responsible for addressing obesity can lead to conflict in the clinical encounter. The model presented in this article describes a shared understanding of roles and responsibilities, and makes suggestions on how primary care can develop obesity services that are acceptable to and appropriate for patients and practitioners.
First, each article was read multiple times to gain familiarity with the subject. ‘First order constructs’ (that is, direct quotes) and study designs were used to contextualise each study. Second, themes were identified and refined as the articles were re-read. Third, the ‘second order constructs’ (that is, authors’ published interpretations of direct quotes) were grouped by theme to create an ‘integrating scheme’ (Table 1). Fourth, this ‘puzzle’20 was used to conduct a ‘reciprocal translation’, whereby the second order constructs were translated into each other (see the section on Narratives). This was done by applying principles of grounded theory, specifically the constant comparison method.21 Novel themes were allowed to emerge iteratively without a priori assumptions, until theoretically saturated.
Integrating scheme: second order constructs and emerged themes
Finally, a lines-of-argument synthesis was applied to derive a novel interpretation of the reciprocal translation.20 It is done by synthesising the lines of arguments identified from the second order constructs (Table 2) into an overarching line of argument (third order construct) that addresses the research question.
Summary of reciprocal translation synthesis
RESULTS
Literature review
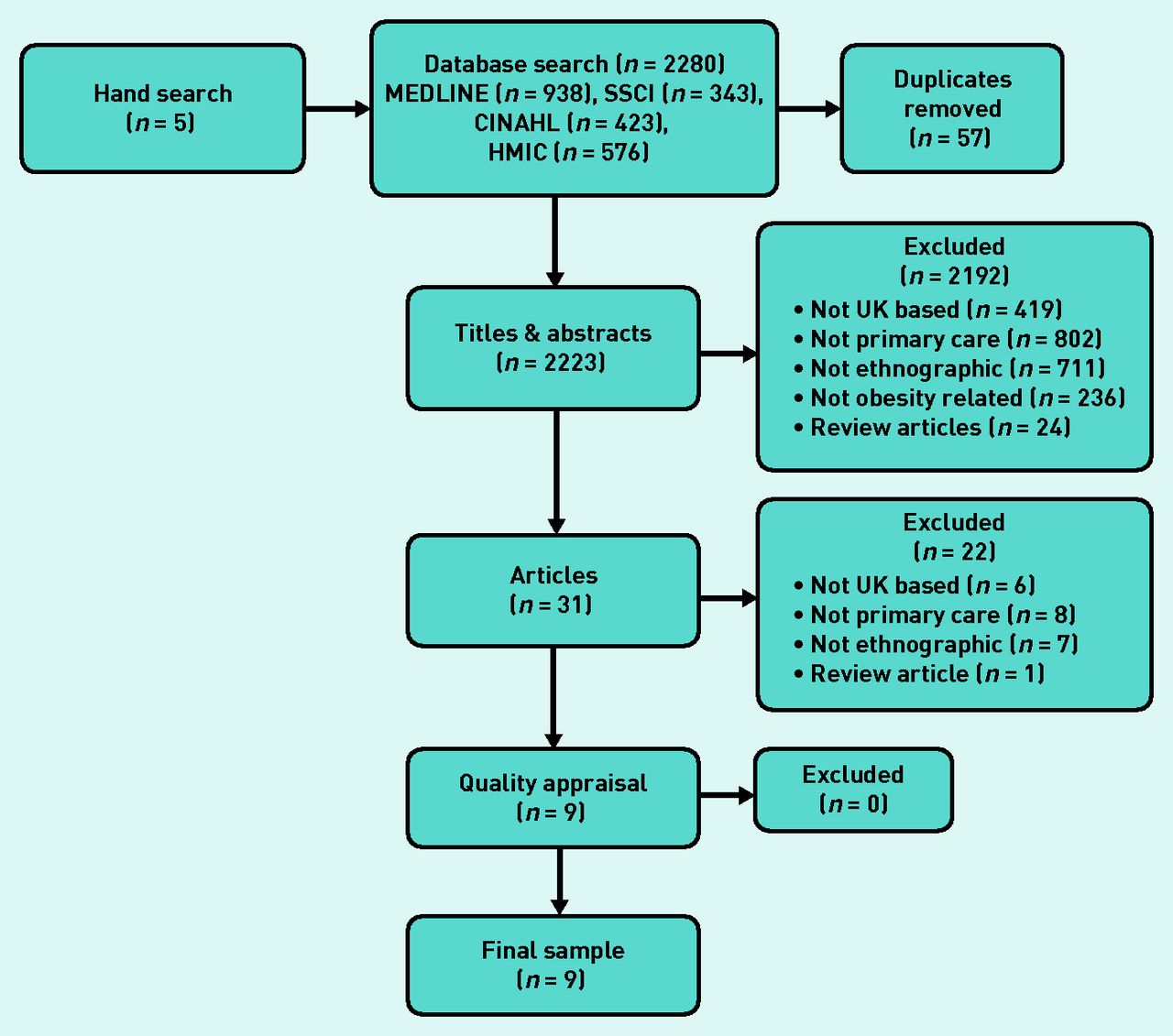
Figure 2 describes the search process. The final sample of studies (n = 9) included perspectives from patients (n = 105) and practitioners (n = 144). One article included both patients and practitioners. Patient studies comprised obese adults receiving treatment (n = 2); parents of overweight children (n = 1); and overweight laypeople (n = 1). Practitioner studies comprised GPs only (n = 1); nurses (practice, district, and health visitors) only (n = 1); and a mix of practitioners (GPs, practice nurses, school nurses, community nurses, health visitors, dieticians, clinical psychologists) (n = 4). Studies were conducted in London (n = 1), south-west England (n = 2), Yorkshire (n = 3), north-east England (n = 1), Glasgow (n = 1), and UK wide (n = 1). All articles were assessed to be moderate to high quality.

Search process and final sample.
HMIC = Health Management Information Consortium.
Reciprocal translation synthesis
Table 1 presents the integrating scheme. Second order constructs were identified from the patient (n = 11) and practitioner (n = 11) studies. Five themes emerged: knowledge/education, medicalisation, uncertainty, communication, and blame/stigma.
The following section presents a narrative of the reciprocal translation syntheses, by patient and practitioner. Table 2 reports the second order lines of arguments, by theme.
Narrative of patient studies
Knowledge/education
Patients reflected the predominant health messages that they are responsible for obesity and need to change their lifestyles.22–25 Barriers to weight loss were identified: lack of resources,23,25 and loss of ‘motivation’ and ‘self-respect’.23 ‘Failure’ can negatively affect confidence and self-esteem.24 Psychological support and individualised advice was often not offered by practitioners, despite clinical recommendations.22,25 Patients found lifestyle advice alone ‘problematic’ because ‘support for continued motivation’ was seen as vital.22,24 Because patient experiences lay within ‘complex’ ‘life stories’, awareness-raising around the socioecological factors influencing obesity could help to promote positive change in patient behaviour.23
Medicalisation
Patients tended to adhere to a biomedical approach, believing obesity is ‘pathological’23 and ‘abnormal’.25 Parents of overweight children felt ‘listened to’ and ‘taken seriously’ if practitioners ran tests for comorbidities.22 Treatment options motivated patients, ‘legitimised’ concerns, and helped them to realise the ‘seriousness of their situation’.25 Obese patients were framed as having ‘more hope than expectation’ for success,24 and hoping for ‘miracle cures’ or ‘magic bullets’.23,24 ‘Stress, low mood and negative emotions’ were identified as causes of weight gain,25 but not wider determinants of obesity.23 Emphasis on the socioecological model may lead to more constructive solutions.23,24
Uncertainty
Some patients lacked confidence in care options, mainly because of observed ineffectiveness.22–25 Patients also doubted practitioners’ ability to deal with obesity, citing a ‘lack of competence’22 or concern over quality.24 Practitioners’ ‘ambivalence’, ‘uneasiness’, and doubts about addressing obesity were perceptible by patients, leading to ‘demoralisation’ and ‘delayed presentation’.25 ‘Mixed feelings’ over the effectiveness of medication and availability of support may reduce service use.24
Communication
‘Successful’ interventions with nurses were reported to be ‘supportive, non-judgemental, relaxed and informal’,25 stemming from ‘interested, positive, and empathetic’ practitioners.22 Some parents of overweight children felt ‘dismissed’, despite the sense of urgency to address obesity.22 Practitioners were perceived to be ‘frustrated’.22 This ‘inappropriate’ care made patients feel ‘resigned’, and to stop seeking care.22 Patients felt ‘disappointed’ by practitioners for not being ‘helpful’ or ‘understanding’.24 Practitioners need training to identify those ‘at risk’ and provide support.25
Blame/stigma
Obese patients concentrated on their own ‘personal failure’, although there was ambivalence between feeling their lifestyles are to blame (for example, ‘laziness’), and factors outside their control (for example, ‘genetics’).23 A sense of ‘blame’24 by practitioners led to a ‘detrimental effect’ on confidence and self-esteem, and a ‘refusal to talk openly’ about lifestyles.25 Fear of ‘judgement’24 was a barrier to enacting lifestyle advice, in particular exercising in public.23,25 Practitioners who do not recognise the ecological factors that influence obesity appear to ‘lack sympathy’.22
Narrative of practitioner studies
Knowledge/education
Many practitioners were unsure of care options, or their effectiveness.26–29 This may be because some practitioners do not consult clinical guidance, or lack obesity-specific training.27,28 However, it is more likely due to the belief that the evidence is not strong enough.26–29 By having limited effective services to offer, practitioners felt ‘powerless’26 and that obesity management was ‘placed on’ them ‘without careful thought’.28 Practitioners identified patients’ poor education and ‘ignorance’ as a barrier to effective change.27–29 Practitioners saw parents as ‘not making the link’ between ‘junk food’ and physical inactivity and obesity.28
Practitioners expected a ‘quick fix’ and became frustrated if patients did not change.23,26,27
Medicalisation
Most practitioners perceived obesity as a ‘social problem’, rather than a medical issue.26–30 Explanations for the causes of obesity included ‘family problems’27–30 (cookery skills5 and time pressures27,28), socioecological barriers (unsafe streets28 and availability of foods23,27,29,30), and ‘deeper social structures’23 (poverty,23,27,30 the media,23,27,28 and societal stigma26,30). Practitioners ‘straddled’ between biomedical and socioecological views of the cause of obesity, holding ‘faith’ in an individual-focused model of care but also acknowledging the need for systemic change.23 Because weight maintenance is complex and raises ‘social’ and ‘personal’ issues, it may be ‘relevant’ for primary care to only involve cases where comorbidities exist, especially for GPs.26,27,29,30 On the other hand, some nurses improved their effectiveness by discussing obesity in medical terms, for example, focusing on health rather than body size.30
Uncertainty
While accepting prevention as part of the practitioner’s role, it remained an ‘unpopular’ aspect of their work27 and it was not clear how to operationalise prevention.29 GPs took a ‘confused world view’, because despite the ‘lack of evidence’ to support obesity interventions, they nonetheless provided obesity services.23 The experience that obesity is ‘extremely challenging’, due to the limitations of primary care, led practitioners to take a ‘fatalistic’ approach, believing that ‘nothing works’.29 GPs were in a ‘state of conflict’ with a sense that patients expected GPs to ‘take ownership’ of patients’ ‘problems’, and a belief that patients are responsible for self-management.26 However, ambivalence can be seen as a ‘realistic stance’ for practitioners; nurses ‘juggled’ their expectation of behaviour change with a ‘non-judgemental approach’.30
Communication
The lack of sufficient evidence was seen as a ‘barrier to even raising the issue’.29 The desire to maintain a positive, ongoing relationship caused practitioners to avoid addressing the ‘sensitive topic’ of obesity,28–30 ‘offending’ patients,26,28 or weakening trust.29,30 Practitioners ‘repeatedly’ cited poor training and communication, and felt they might be ‘professionally unprepared’.23 Practitioners’ ‘awkwardness’30 about or ‘frustration’27 over obesity negatively affected patient satisfaction with services,30 and may counter potentially ‘positive’ interactions, such as motivational interviewing.27
Better training in counselling techniques is required23,27,28,30 including ‘patient-centred’ and ‘non-judgemental’ approaches, with awareness of the psychological and social aspects of obesity.23,30 High levels of GP involvement may not be feasible but regular contact with other practitioners such as nurses is important to ‘instil confidence’ and take a ‘team approach’.27
Blame/stigma
This theme stood as a culmination of the previous themes of knowledge, medicalisation, uncertainty, and communication. Practitioners believe obese patients are ‘in denial’,26–30 get ‘offended’,27,30 ‘prickly’,29 ‘nasty’,28 or feel blamed28 when the topic is broached. Stigmatising language was used to describe patients: ‘clueless’,26 ‘brainwashed’,23 and ‘hopeless’,28 and rather they should be ‘cooperative’28 and ‘enthusiastic’.27
Practitioners who maintain awareness of obesity-related stigma26,30 and their own ambivalence30 may help improve the patient–practitioner relationship. Empathic26,27,30 ‘patient-focused’30 and ‘non-judgemental’30 approaches are recommended. Emphasis should be on socioecological determinants of obesity to reduce patients’ ‘unhappiness’ and ‘negative feelings’, thus leading to more constructive solutions.23
Box 1 summarises the above discussion of the reciprocal translation in a two-by-two matrix. It is divided by:
Patient perspectives of their own roles.
Patient perspectives of practitioners’ roles.
Practitioner perspectives of patients’ roles.
Practitioner perspectives of their own roles.
Matrix of the reciprocal translation synthesis summarising roles and responsibilities in lifestyle change assigned by patients and practitioners
| Actors’ roles and responsibilities | |||
|---|---|---|---|
| Patient | Practitioner | ||
| Responders’ beliefs | Patient | Responsible for a biomedical issue | Provide support for biomedical issues and psychological/‘personal’ issues |
| Ineffective in making change | Determine and communicate respective roles | ||
| Resigned and frustrated Stigmatised | |||
| Practitioner | Change behaviours | Be involved only where evidence is strong | |
| Self-motivate and have ‘willpower’ | Responsible for medical problems; minimise ‘dealing with personal’ issues | ||
| Responsible for psychological/‘personal’ issues | Resigned and frustrated | ||
Lines-of-argument synthesis
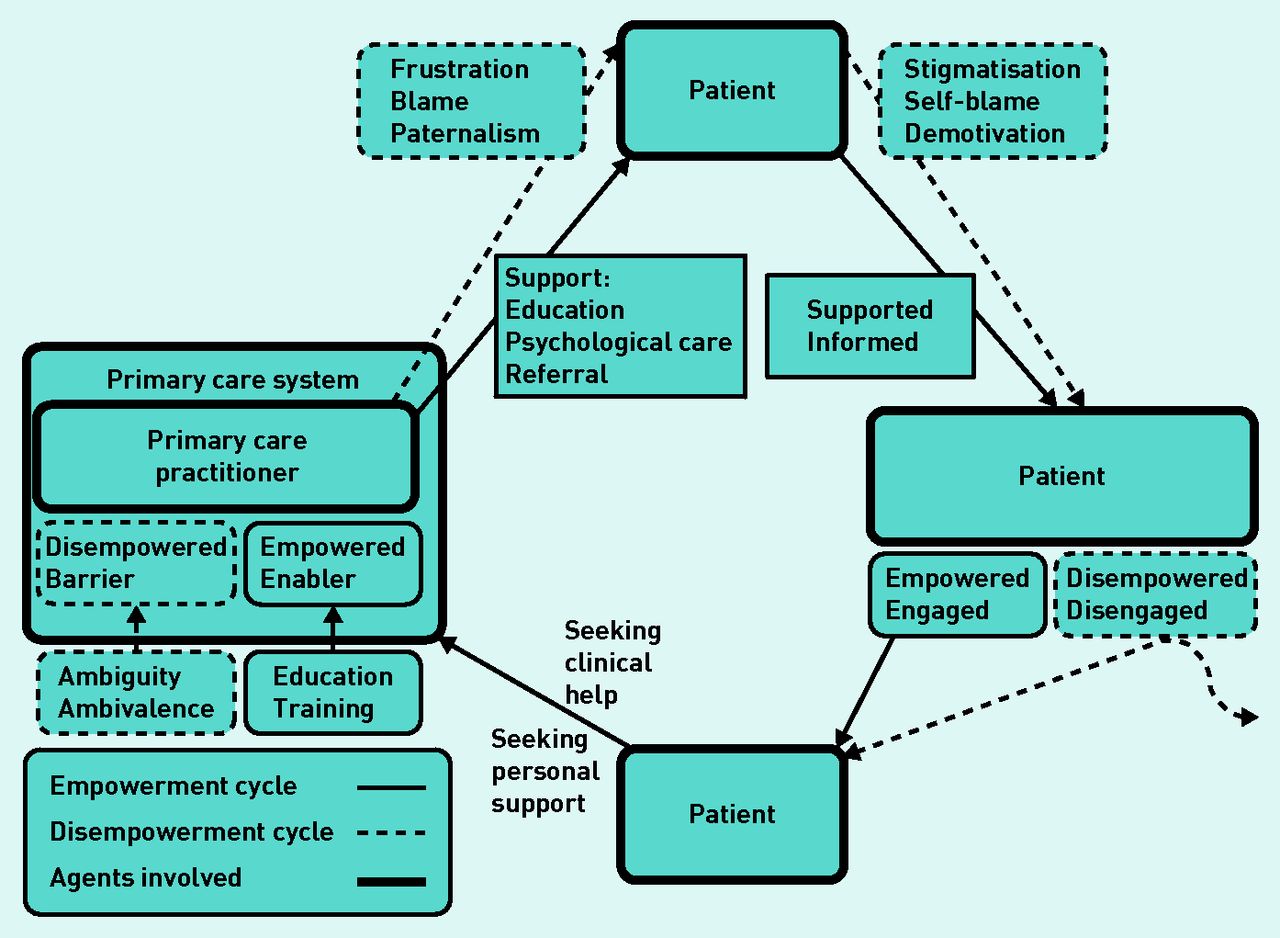
Figure 3 depicts a model of the overarching lines of argument on roles and responsibilities in how to address obesity in the primary care setting. The model describes an ‘empowerment cycle’ and a ‘disempowerment cycle’. As a patient engages with primary care, they will encounter one of two types of practitioner.
One is the disempowered practitioner who is ambivalent and ambiguous, and stands as a barrier to obesity services. Practitioners viewing patients as ‘uncooperative’ or ‘defensive’ may misinterpret patients’ mistrust and sense of being singled out or stigmatised. The patient in this case is disempowered and less likely to engage in future health services.

{kind=link}
{kind=link}
{kind=link}
Lines-of-argument model: cycles of empowerment and disempowerment involved in addressing obesity in primary care.
The second is the practitioner empowered through the primary care system, with training and a sense of how to address obesity. The patient will receive support, in the form of education, non-judgemental care, or service referral. The sense of being supported and knowing what to expect from primary care empowers the patient, and leads to increased engagement with health services.
DISCUSSION
Summary
This study synthesised patient and practitioner perspectives on how obesity should be addressed in primary care in the UK. It identified an intricate interplay between patients and practitioners, with the empowerment of patients to access health services reliant on the empowerment of practitioners to take an unambiguous position.
Strengths and limitations
The NHS’s assessment of meta-ethnography indicates the method has potential to effectively synthesise qualitative research and generate evidence, which the present study attempts to do.15 The sample comprised the desired diversity in criteria, and although small, the size enabled an examination of study context, an accepted strength of meta-ethnography.15 Thus, the model does not purport to be definitive and represent all practitioners, but is one based on the author’s subjective interpretations.
Comparison with existing literature
Where there is uncertainty of how to address obesity, practitioners can ‘lack authority’.31 Despite this, patients still look to practitioners for support, reflecting previous theoretical analyses of the public’s ambivalence between the power and limitations of modern medicine.32 Clinical guidance allows for professional-led practice in the primary care setting.5 Martin and Learmonth33 warn against a ‘gap between everyday organisational realities and the pronouncement of policymakers’, and advocate pluralistic leadership between policy, practice, and patients. However, in the case of obesity interventions in primary care, the aspirational ‘bottom-up’ approach may leave the profession vulnerable to ambiguity and ambivalence.
The internalisation of obesity-related blame and stigma can have detrimental effects on patients’ self-esteem and social networks, which can result in further weight gain.34 Conversely, evidence is growing for the positive potential of clinical ‘placebo effects’ on depression, anxiety, and pain, the mechanism for which is follow-up and continuity in care.35 Moerman and Jonas36 describe this as the ‘meaning response’, because, whereas placebo is inert, care is interpreted by patients with context-specific, cultural meanings. This phenomenon supports the recommended patient-centred models of care; however, practitioner performance is still measured by diagnosis, not individual context.37
Finally, the socioecological model of obesity has potential to improve the effectiveness of primary care in addressing obesity, through an understanding of the day-to-day challenges of a potentially physically and psychologically debilitating condition. The biomedical model of obesity alone does not explain why people have poor diets or low activity levels. Indeed, empowerment must be framed within the context of individual lived experiences of inequalities, and subsequent roles in society, in order for it to adequately address issues of power.38
Implications for research and practice
Future work should focus on implementation of the theoretically-based model presented here, which could be tested and advanced through theoretical and empirical research. The model could be used to develop effective obesity-related curricula for students and continuing professional development. The study could be repeated on other health systems to share learning, and gain cross-cultural understandings of how responsibility for obesity is constructed.
The English government formerly adopted the ‘nudge model’,39 in the form of the Behavioural Insights Unit and the Responsibility Deal, into its most recent obesity policy, ‘to help people to make better choices … rather than reducing choice’.12 The BMA criticised it as ‘inadequate ... likely to entrench existing inequalities’.4 This top-down approach risks disempowering people by exerting authority with one hand (that is telling people how ‘best’ to behave) and placing responsibility on individuals with the other (for example, not requiring a reduction in unhealthy options). Policy inroads have been made, with the ‘statement for action’ by health professionals to reduce obesity-related inequalities,40 and the Academy of Medical Royal Colleges’41 recommendation to train professionals in ‘sensitive recognition and appropriate referral’. Approaches to obesity that engage all actors including the public — such as knowledge exchange, which bridges research, policy, and practice42 — are needed to co-produce context-specific solutions to a complex health issue.
Acknowledgments
The author thanks Mrs Yitka Graham for her assistance searching the literature databases, and Professor Greg Rubin and Dr Silvia Scalabrini for their comments on earlier drafts.
Notes
Funding
This work was funded with support from the Wolfson Research Institute for Health and Wellbeing, at Durham University.
Ethical approval
Ethical approval was not sought for this literature review and synthesis.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The author has declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received September 22, 2014.
- Revision requested October 21, 2014.
- Accepted October 29, 2014.
- © British Journal of General Practice 2015
REFERENCES
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

