


Abstract
Background The care that most people receive at the end of their lives is provided not by specialist palliative care professionals but by generalists such as GPs, district nurses and others who have not undertaken specialist training in palliative care. A key focus of recent UK policy is improving partnership working across the spectrum of palliative care provision. However there is little evidence to suggest factors which support collaborative working between specialist and generalist palliative care providers
Aim To explore factors that support partnership working between specialist and generalist palliative care providers.
Design Systematic review.
Method A systematic review of studies relating to partnership working between specialist and generalist palliative care providers was undertaken. Six electronic databases were searched for papers published up until January 2011.
Results Of the 159 articles initially identified, 22 papers met the criteria for inclusion. Factors supporting good partnership working included: good communication between providers; clear definition of roles and responsibilities; opportunities for shared learning and education; appropriate and timely access to specialist palliative care services; and coordinated care.
Conclusion Multiple examples exist of good partnership working between specialist and generalist providers; however, there is little consistency regarding how models of collaborative working are developed, and which models are most effective. Little is known about the direct impact of collaborative working on patient outcomes. Further research is required to gain the direct perspectives of health professionals and patients regarding collaborative working in palliative care, and to develop appropriate and cost-effective models for partnership working.
INTRODUCTION
The need to increase the numbers of health professionals involved in palliative and end-of-life care has become a priority of palliative care policies across the developed world. Ageing nations and expanding populations mean annual numbers of deaths are predicted to rise by as much as 17 per cent over coming years.1 In the UK, the recent palliative care funding review has estimated that, currently, up to 457 000 people need access to a palliative care, but around 92 000 people are not being reached.2 In the UK in 2009, there were 507 specialist palliative care inpatient services, whose remit is to care for patients who require continuous or high levels of support;3 however, the care that most people receive at the end of their lives is provided not by specialists but by generalists, such as GPs, district nurses, nursing home staff, hospital staff, and others who have not undertaken specialist palliative care training.4
Generalist palliative care provision has seen limited research attention to date. There is no consensus regarding the definition of the term ‘generalist’ in the context of palliative care,4 and people have reported differing understandings of the purpose and scope of generalist palliative care;5,6 in spite of this, international health policy has sought to place the generalist at the heart of palliative care provision.7,8 In the UK, recent policy has highlighted the importance of training and education for generalist providers if they are to provide effective palliative care.9 However, difficulties incorporating palliative care into a generalist workload have been reported, as has defining the role of palliative care outside the specialist setting.10,11 A recent study by Gott et al reported significant challenges in generalist working in England and New Zealand. Difficulties with defining the nature and limits of generalist palliative care, as well as negotiating partnership working were reported; these reveal a significant gap between palliative care provision as enshrined in policy and the reality reported by frontline staff.6
A key focus of UK policy is improving communication, partnership working, and multidisciplinary involvement across the spectrum of palliative care provision.9 Although good communication and improved partnership working between specialist and generalist providers have been identified as facilitators for optimum palliative care provision,12 there is little evidence to suggest which factors support these working relationships. In addition, partnerships have costs in terms of negotiating, developing and maintaining working relationships, and translating these into successful outcomes.13
The current economic climate makes significant expansion of palliative care services unlikely, yet policymakers have highlighted a commitment to ensuring high-quality palliative care for all.7,9 As such, identifying factors that support effective partnership working between generalist and specialist providers of palliative care is not only timely, but also crucial for improving patient care. This study aimed to carry out a systematic review of factors supporting good partnership working between generalist and specialist palliative care providers.
How this fits in
A key focus of UK policy is improving partnership working across the spectrum of palliative care provision. This systematic review identifies factors supporting partnership working between specialist and generalist palliative care providers, and provides clinicians with examples of successful partnership working models. Further research is required to generate a better understanding of partnership working, and to identify and evaluate appropriate outcome measures.
METHOD
Design
A systematic review was undertaken to explore factors supporting good partnership working between generalist and specialist providers of palliative care. The review synthesised evidence from a variety of sources and included quantitative, qualitative, and grey literature,14 and was undertaken in the following stages:
Development of a search strategy and inclusion criteria;
Assessment of relevance; and
Data extraction and synthesis, using a descriptive thematic model.
Search strategy and inclusion criteria
The aim of the search was to identify a comprehensive list of literature that met predefined inclusion criteria. An initial scoping search was undertaken to identify and evaluate search terms. Medical Subject Headings and keywords were identified, and relevant databases selected and searched using the search terms highlighted in Box 1. The databases MEDLINE, Embase, CINAHL, Cochrane, PsychINFO, and Web of Science were searched for literature published until January 2011. Grey literature searches were conducted in the above databases and using internet search engines. Relevant references from bibliographies and citations were followed up.
Box 1. Search terms
End-of-life terms
Terminally ill; end of life; end-of-life; last year of life; palliative; hospice; terminal care; terminal patient; supportive care
Specialist care provider terms
Palliative service; palliative care service; (palliative and (expert or specialist)); palliative care team; palliative medicine; palliative care consultant; palliative doctor; palliative care nurse; Macmillan nurse; Marie Curie nurse
Generalist provider terms
Primary care physician; family doctor; general practitioner; GP; Community Health Nursing/or Public Health Nursing; district nurse; community matron; community nurse; Homes for the Aged/or aged residential care/or Nursing Homes; care home; residential home; nursing home
Partnership and collaboration terms
Partnership working; collaboration or cooperative behaviour; collaborative working; communication; shared working; joint working; shared care; inter-agency collaboration; extended team.
To comply with the inclusion criteria, studies had to:
relate to factors affecting collaborative or partnership working between generalist and specialist providers of care;
relate to palliative or end-of-life care in adults;
be empirical; and
be written in English (resource restrictions prevented the translation of non-English-language papers).
For the purposes of this review ‘specialist’ providers were defined as health and allied health professionals with specialist or accredited training in palliative care delivery, and ‘generalist’ providers as health professionals with no specialist or accredited training in palliative care. These definitions are in line with The End of Life Care Strategy for England.7
Assessment of relevance
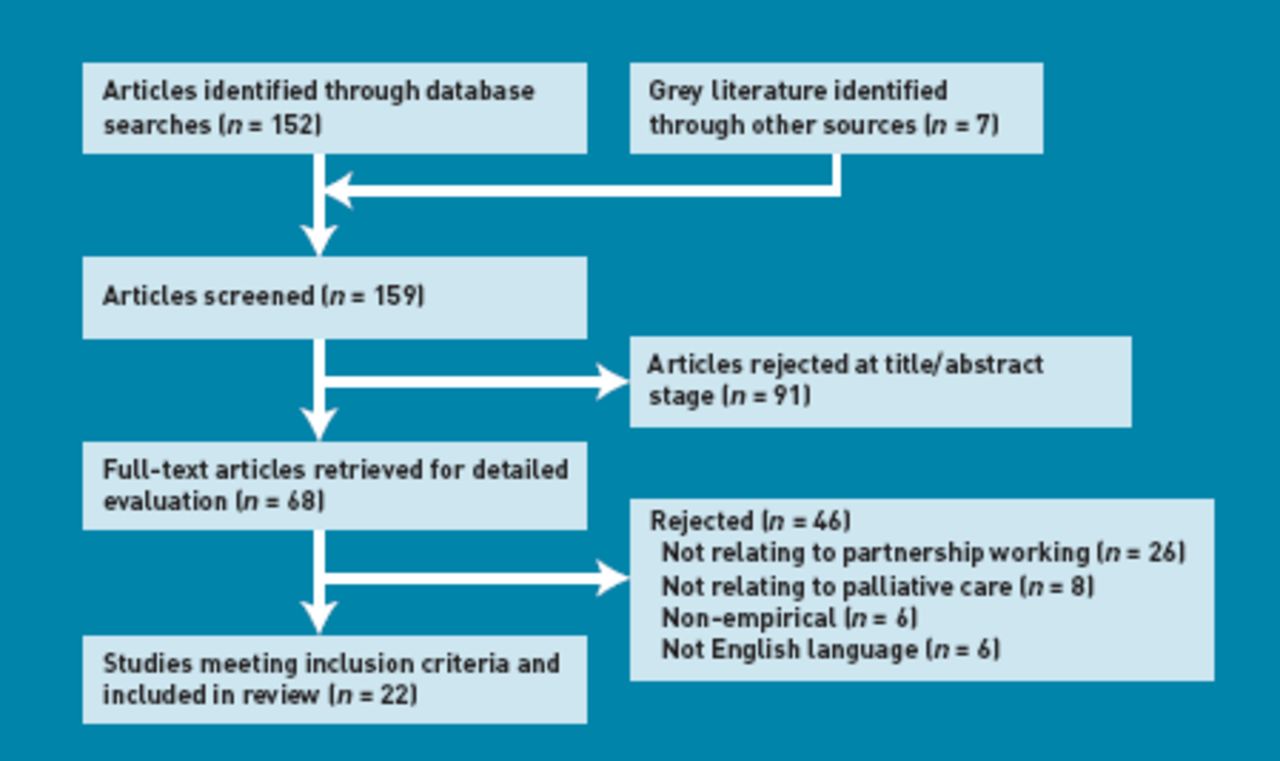
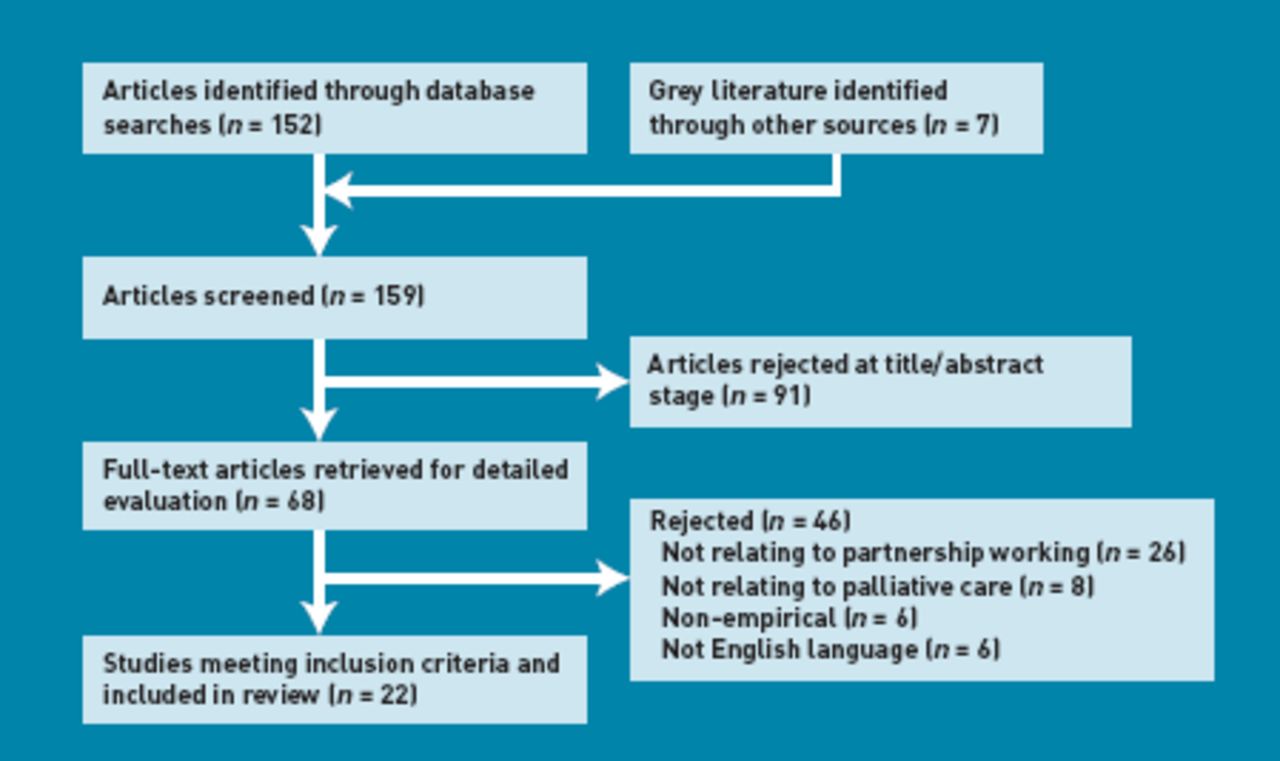
The search resulted in 159 papers being identified. Study selection was conducted in a systematic sifting process over three stages: title, abstract, and full text (Figure 1). Full texts were extracted for 68 papers, each of which was independently reviewed by two researchers; 46 papers were rejected. Where there was disagreement between reviewers, consensus was reached through discussion. In total, 22 papers satisfying the inclusion criteria were identified;5,15–35 these are detailed in Table 1.
{kind=link}
PRISMA diagram of included literature.
Papers included in the review
Data extraction and synthesis
As it was anticipated that a range of papers using different methodologies would be obtained, the review was conducted using a descriptive thematic method for systematically reviewing and synthesising research from different paradigms. Thematic analysis offers advantages, including allowing clear identification of prominent themes, and providing organised and structured ways of dealing with the literature.36 The thematic approach was data driven; major or recurrent themes relating to partnership or collaborative working were identified in the literature and the findings of the primary studies were summarised under these headings. Within each theme, both supporting and conflicting data were reported, if available. No attempts were made to quantitatively summarise and synthesise study quality, due to the recognised methodological problems with this approach when combining qualitative and quantitative evidence.36,37 These include heterogeneity of study purpose and study design, and lack of numerical data in qualitative studies.
RESULTS
The 22 papers included in the review represented an international perspective; 13 papers were from the UK, seven from Australia, one from New Zealand, and one from Canada (Table 1). Eleven papers were concerned with exploring factors involved in, or attitudes to, partnership working.5,15,17,20,21,24,28,31,33–35 six were descriptions of the development or implementation of partnership working models.16,18,19,22,25,30 and five were evaluations of partnership working models.23,26,27,29,32 Eleven of the papers used qualitative methods;5,15,17,20,21,24,28,30,31,33,34 seven used quantitative methods;19,22,23,25,27,29,35 three used mixed methods;18,26,32 and one used a case-study approach.16
Some methodological weaknesses exist in the studies reviewed, so some caution must be exercised when attempting to draw any firm conclusions. Only one of the studies was a randomised controlled trial and most evidence was derived from sources that do not enable generalisability. Analysis of the data led to the emergence of five key factors that could enhance partnership working between specialist and generalist palliative care providers:
Good communication between providers;
Opportunities for education;
Clear definition of roles and responsibilities;
Access to specialist palliative care; and
Coordinated and continuous support.
Good communication between providers
Communication between specialist and generalist providers was a feature of many of the included studies. The evidence suggests that existing communication strategies are not necessarily appropriate, timely, or relevant. Good communication between teams was a key feature of the successful implementation of collaborative working models.17,19 Examples of good communication strategies that were reported included heart failure nurses being invited to attend community palliative care multidisciplinary team meetings,18 liaison links being established between care home staff and a local hospice,22 and case conferences being held between GPs and specialist palliative care providers.27
Poor communication was cited as a factor that prevented generalist staff from becoming more involved in palliative care.24,31 Encouraging dialogue between specialities was identified as an important future priority.21 Identified barriers to effective communication included a lack of processes for communication,35 and issues establishing networks. Good communication networks are often the result of personal liaison rather than systematic processes.33
Opportunities for education
Education and training were identified as important facilitators of collaborative working, with the many of studies identifying education for generalists as a particular priority.19,23,24–26,28 Examples of successful education models for generalists included study days for care home staff,22 practice-based education and decision support for GPs,25 and educational inductions for palliative care partnership models involving GPs and practice nurses.26 One study reported shared learning practices involving both specialists and generalists: as part of the evolution of joint working between heart failure and specialist palliative care staff, heart failure nurses attended formal education events organised by specialist palliative care services and vice versa, which was successful in facilitating shared learning.18
Increased education was not seen as necessary in all studies: O'Connor and Lee-Steere reported that some rural GPs did not see the lack of training in palliative care as a problem.28
Clear definition of roles and responsibilities
A need for clarification regarding the roles and responsibilities of specialist and generalist providers was identified as a priority. Misunderstandings regarding roles and responsibilities were found to have a negative impact on: effective partnership working; the degree of interaction between specialist and generalist colleagues; and the readiness of professionals to engage in partnership working.15,17,20,21,35,30 In a national consultation on generalist palliative care provision, separation of responsibility was identified as a significant barrier to collaborative working.31 Alsop identified that any model for collaborative working should also clarify definitions and terminologies to reflect the roles and responsibilities of different specialist and generalist services.16 Professional territorialism — an unspoken demarcation between health professionals, regarding who coordinates and provides patient care — was also identified as a barrier to effective partnership working.17,33 Professional territorialism may result in difficulties negotiating relationships, power issues,34 and concerns about deskilling generalist staff.20,29
Access to specialist palliative care
Appropriate and timely access to specialist palliative care services was seen as crucial to effective partnership working and was shown to support generalists in providing sustainable care.5,26 Regular contact and liaison with a hospice,22 a flexible service from specialist palliative care providers,29 and visibility of specialist palliative care services in hospital5 were all reported as enhancing the capacity of generalists to deliver effective palliative care. Generalists identified good out-of-hours care and access to round-the-clock support from specialist palliative care services as being key aspects of successful partnership working.22,24,25,28 Specialist palliative care telephone consultation services for generalists were viewed positively in a number of studies exploring models of palliative care collaboration in the community.18,22,28 Difficulty accessing specialist palliative care services was identified as a factor preventing GPs from becoming more involved in palliative care.24
Coordinated and continuous support
Coordinated patient care and continuous support were identified as important outcomes of successful partnership working. Achieving coordinated care and continuous support for patients was seen as challenging, and different models were proposed for ensuring continuity of care.32 In one study, heart failure nurses took on the role as coordinating key workers for their patients with heart failure. The model was evaluated as both cost effective and sustainable.18 A study by Blackford and Street found that palliative care nurse consultants played an important role in facilitating continuity of care across healthcare services.17 A lack of consensus about who has coordinating responsibility for patients,33 the development of care plans in isolation from other teams,35 and poor coordination between teams21 were all found to impede continuity of care and effective coordination of care.
DISCUSSION
The studies described in this article provide a range of examples of good partnership working between specialist and generalist palliative care providers. The evidence suggests that successful collaborative working models can have several positive outcomes. These include positive impacts on patients such as more patients dying in their place of preference,19,29 and improved patient education and better symptom management.30 Successful collaborative working models have been shown to be cost effective, and do not lead to excess burden on specialist palliative care services.18 Enhanced partnership working also has significant positive impacts for health professionals, including empowering generalists, supporting staff in decision making, and increasing positive attitudes among generalists to specialist palliative care provision.32 These findings are in line with other research that highlights a range of positive outcomes of multidisciplinary working in other areas of healthcare delivery.38
Strengths and limitations
This review addresses a gap in the evidence by identifying a range of factors supporting partnership working between generalist and specialist palliative care providers. Comprehensive electronic search, retrieval, and review strategies were used. However, this study's searches are subject to some limitations, as principally English language databases were used and, due to time and resource limitations, hand-searches of journals were not completed and experts in the field were not contacted directly. As such, some studies may have been missed.
Comparison with existing literature
Evidence from this review suggests that a significant barrier to good partnership working is a lack of clear definition regarding the roles and responsibilities of both generalist and specialist providers. A lack of clearly defined terminology has been well recognised as an issue in the palliative care literature,11,39,40 and a lack of consensus regarding definitions has been described as a fundamental problem in the field.39 Although there is a growing recognition that palliative care provision needs to be integrated into the practice of generalists,9 clearly defined roles have yet to be agreed. Roles, responsibilities, and definitions require clarification to minimise the separation of responsibility and to improve decision making in palliative care collaborative working models.
Education and training were highlighted as important facilitators of successful partnership working. However, the majority of studies in this review focused on educational opportunities for generalists; findings regarding efficacy and acceptability were mixed. Evidence has suggested that education alone may be insufficient to effect culture change among health professionals,41 so initiatives that more effectively moderate attitudes and behaviour should be explored. Opportunities for education involving shared learning may be more effective in engaging health professionals and facilitating learning.18 Further research should seek to explore models of shared learning more formally to facilitate education across disciplines.
Contact and liaison with specialist palliative care services, and timely access to them, are important features of successful partnership working. Good communication is a key component of improved access to specialist palliative care. Models of partnership working, therefore, need to develop strategies to enhance communication between different groups and facilitate formalised routes of access between specialists and generalists. The evidence suggests that communication may, more often, result from personal liaison rather than formal processes;33 successful routes of communication should be examined for common features to generate evidence that can facilitate formal communication and enhance access to specialist palliative care.
Achieving coordinated and continuous support for patients at the end of life is an important outcome of successful partnership working. Patients have reported continuity of care and an individualised approach as some of the most important features of good palliative care42 but continuity of care can be difficult to achieve when many agencies are involved in providing an individual package of care.43 Studies involving GP facilitators, key workers, and link nurses have met with mixed success, and barriers to achieving continuity of care include the difficulty that exists in liaising between different services and accessing specialist palliative care. Further research is needed to explore ways in which continuity of care can be successfully achieved and to ascertain patient outcomes as a result of coordinated care between specialists and generalists.
Implications for practice
The evidence suggests that, although there are a range of strategies for enhancing collaborative working between specialists and generalists, these are often the result of informal interactions rather than systematic processes. Although 11 of the included studies described the development or evaluation of a formal model of collaborative working, those models varied widely in their aims, processes, and intended outcomes.16,18,19,22,23,25–27,29,30,32 There is little consistency in the way models are developed and their success evaluated.
There is a clear need to undertake empirical research to generate a deeper understanding of factors mediating partnership working in palliative care. In addition, research should explore the direct effects of partnership working on patient outcomes and experience, and should seek to identify further appropriate outcome measures for formally evaluating models of partnership working. Outcome measures may include those reported by patients or carers, as well as perceived staff competency in communication and coordinated care delivery. Finally, research should aim to identify the most cost-effective methods of partnership working models and integrated care packages, in order to stimulate service provision across disciplines and improve patient outcomes.2
Notes
Funding
Cancer Experiences Collaborative (CECO).
Ethics committee
No ethical approval required.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article on the Discussion Forum: http://www.rcgp.org.uk/bjgp-discuss
- Received August 25, 2011.
- Revision received September 21, 2011.
- Accepted October 10, 2011.
- © British Journal of General Practice 2012
REFERENCES
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

