Article Text

Abstract
Objective To describe current practice among European paediatricians regarding diagnosis and management of urinary tract infections in children aged 1–36 months and to compare these practices with recently published guidelines.
Design Web-based large scale survey evaluating knowledge of, attitudes towards and the methods for diagnosing, treating and managing urinary tract infections in children.
Setting Primary and secondary care practices in Europe.
Sample 1129 paediatricians.
Results A diagnosis of urinary tract infection is considered by 62% of the respondents in children aged 1–36 months with unexplained fever. The preferred method of urine collection is use of a bag (53% for infants <3 months and 59% for children 4–36 months of age). 60% of paediatricians agree that oral and parenteral antibiotics have equal efficacy. Co-amoxiclav is the antibiotic of choice for 41% of participants, while 9% prescribe amoxicillin. 80% of respondents prescribe ultrasound in all children with a confirmed urinary tract infection. 63% of respondents prescribe a cystography when abnormalities are revealed during ultrasound evaluation. A quarter of respondents recommend antibiotic prophylaxis for all children with any vesicoureteral reflux. The data among European countries are very heterogeneous. The three most recent urinary tract infection guidelines (the National Institute for Health and Care Excellence (NICE), the American Academy of Paediatrics and the Italian Society of Paediatric Nephrology) are not followed properly.
Conclusions Management of febrile urinary tract infections remains controversial and heterogeneous in Europe. Simple, short, practical and easy-to-remember guidelines and educational strategies to ensure their implementation should be developed.
- Nephrology
- General Paediatrics
Statistics from Altmetric.com
What is already known on this topic
-
Management of childhood urinary tract infections in primary care is challenging because early recognition can be problematic, symptoms unspecific and urine samples difficult to obtain.
-
Attitudes towards imaging and prevention of relapse have changed in recent times.
-
Various national and international guidelines with contradictory recommendations have been published.
What this study adds
-
There is marked heterogeneity among European countries.
-
Several discrepancies between best practice guidelines and reality regarding the diagnosis and management of urinary tract infections in children aged 1–36 months are evident.
-
The development of simple, short, practical and easy-to-remember guidelines and of educational strategies to ensure their implementation is necessary.
Introduction
Urinary tract infections (UTIs) are common during childhood and, when fever is present, can be a serious clinical condition. The frequency of UTIs varies according to age, ethnicity, sex and circumcision status, with overall prevalence estimated to be approximately 7% in young children with unexplained fever.1–3
The management of UTIs in primary care is challenging because early recognition can be problematic, as symptoms may not be specific and urine samples can be difficult to obtain. Furthermore, management, including diagnosis, radiological investigations and the use of antibiotic therapy, remains controversial because of a lack of consensus.4
Recently, the National Institute for Health and Care Excellence (NICE), the American Academy of Paediatrics (AAP) and the Italian Society of Paediatric Nephrology (ISPN) published independent updated guidelines.5–7 However, there is a lack of agreement regarding how to perform urine collection, when to perform ultrasound (US) and a micturating cystourethrogram (MCU), and when to use antibiotic prophylaxis (table 1). The main discrepancy concerning the approach after a first UTI relates to the uncertainty regarding the long-term clinical significance of vesicoureteral reflux (VUR) and UTI-related renal scarring.8–12 Moreover, the NICE and some of the ISPN guidelines are complex and hard to remember in detail in everyday clinical practice.
Comparison between guidelines and current practice for urine collection, MCU and antibiotic prophylaxis for VUR
The aim of this study was to describe current practice among European paediatricians working in primary and/or secondary care with regard to the diagnosis and management of UTIs in children aged 1–36 months and to compare these practices with the recently published guidelines.
Material and methods
Questionnaire design
A questionnaire evaluating knowledge of, attitudes towards and methods for diagnosing, treating and managing UTIs in children was developed. The questionnaire included the following sections: demographic characteristics; knowledge of and attitude towards UTI diagnosis; and attitude and practices regarding the management of UTI. It is available in the online supplementary appendix.
The questionnaire was pretested by the national coordinators of EAPRASnet, and modified in light of their comments. EAPRASnet is the European Academy of Paediatrics (EAP) Research in Ambulatory Setting Network, and was established in 2008 by the EAP.13–16
Data collection
Data were collected using a web-based programme available on the home page of the EAP. Respondents were invited to participate via email using a mailing list that had been created for previous EAPRASnet projects. Paediatricians not belonging to the network were prompted by national EAPRASnet coordinators to complete the survey. Three reminders were sent out via email, and data were collected from 25 February until 7 April 2013.
Statistical analysis
All variables were analysed descriptively. Continuous variables are reported as means±SD and categorical variables are presented as frequencies and percentages. All analyses were performed using SPSS V.21 (Chicago, Illinois, USA).
Results
Respondent characteristics
A total of 1601 European EAPRASnet members (European primary care paediatricians) are registered in our system. The web-based questionnaire was answered by 1206 paediatricians. After data cleaning, 1129 valid responses were available for analysis. The response rate was 71%.
Respondents were from 26 European countries, predominantly Italy, Poland, Spain, Austria, Cyprus, Israel, Switzerland and Germany (23%, 19%, 16%, 6%, 6%, 5%, 5% and 4%, respectively). The mean age of respondents was 50 years (±10). The majority of respondents (91%) were primary care paediatricians, who generally deal with pyrexial children. Twenty-four per cent of respondents work in the private sector, 55% in the public sector and 21% in both.
Clinical data
Overall, 62% (697 out of 1129) of the respondents consider a diagnosis of UTI in children aged 1–36 months with unexplained fever, while 21.8% and 15.5% consider it only in children younger than 24 and 12 months, respectively.
Symptoms suggesting UTI were mainly fever (99%), abdominal pain (87%), dysuria and cloudy urine (83%), haematuria and vomiting (81%), frequency (75%) and urgency (71%).
Paediatricians were asked to identify risk factors for UTI from a list of potential indicators. Predisposing factors were: constipation (77%), a family history of VUR or renal disease (86%) and wiping (cleaning/washing) from back to front (88%). Fifty per cent of respondents agreed that circumcised boys were three times less likely to contract a UTI, while 24% did not agree and 26% did not know.
Urine collection
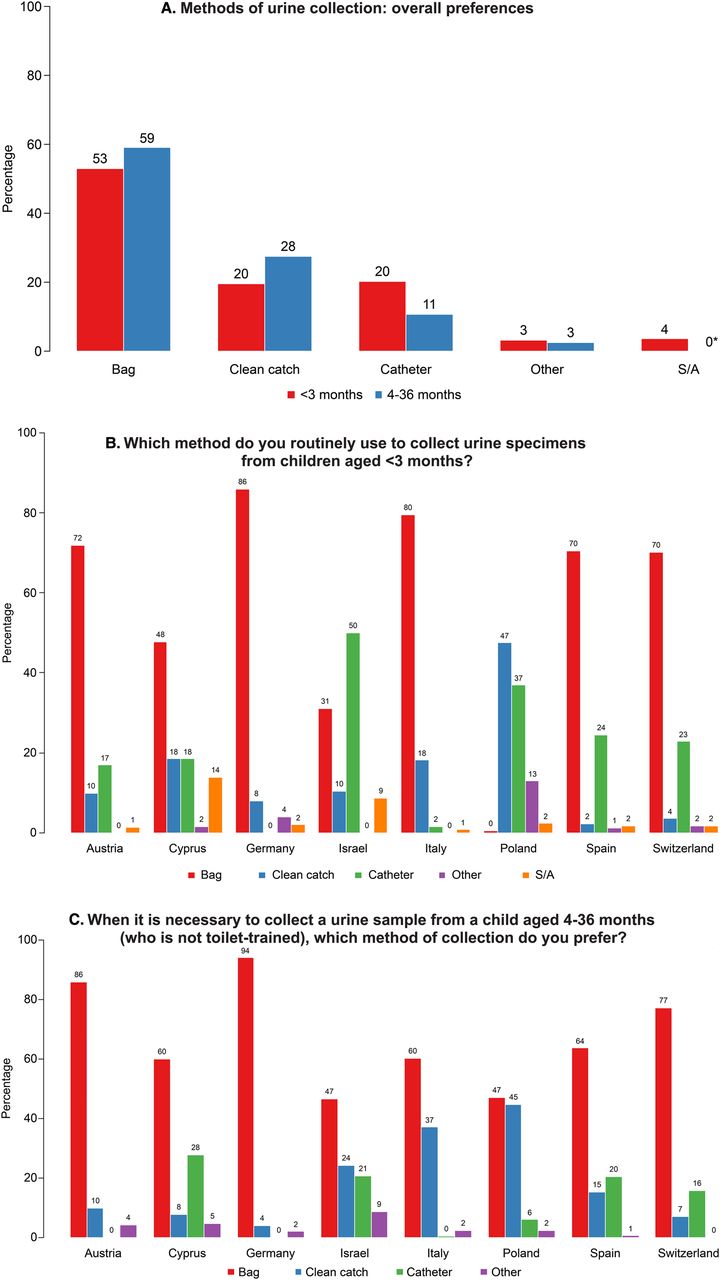
Methods of urine collection are presented in figure 1A. In table 1, the recommendations of the three most recent guidelines are compared, and non-adherence is highlighted.

Methods of urine collection. Overall results (A) and data from the eight most representative countries in children <3 months of age (B) and 4–36 months of age (C). S/A, suprapubic aspiration.
There are major differences among countries, as shown in figure 1B, C and in the tables in the online supplementary appendix. In Germany, for instance, bag use predominates even for children under 3 months of age, while in Poland a bag is hardly ever used. Respondents from both Poland and Italy prefer the clean catch method for children over 3 months of age.
Urine testing
The majority (74%) of respondents use a urinary dipstick to diagnose UTI: nitrites and white blood cell count are the dipstick parameters universally (97%) utilised. However, 54% and 30% of paediatricians, respectively, consider red blood cell count and pH value to be UTI indicators.
Antibiotic treatment
Sixty per cent of paediatricians agree that oral and parenteral antibiotic treatments are of equal efficacy. However, major differences between countries are once again evident (figure 2B) ranging from 90% agreement in Italy to 38% in Germany and Poland. The antibiotic of choice is reported in figure 2A, with 41% preferring co-amoxiclav and almost 10% amoxicillin. Differences among countries can be seen in figure 2B.
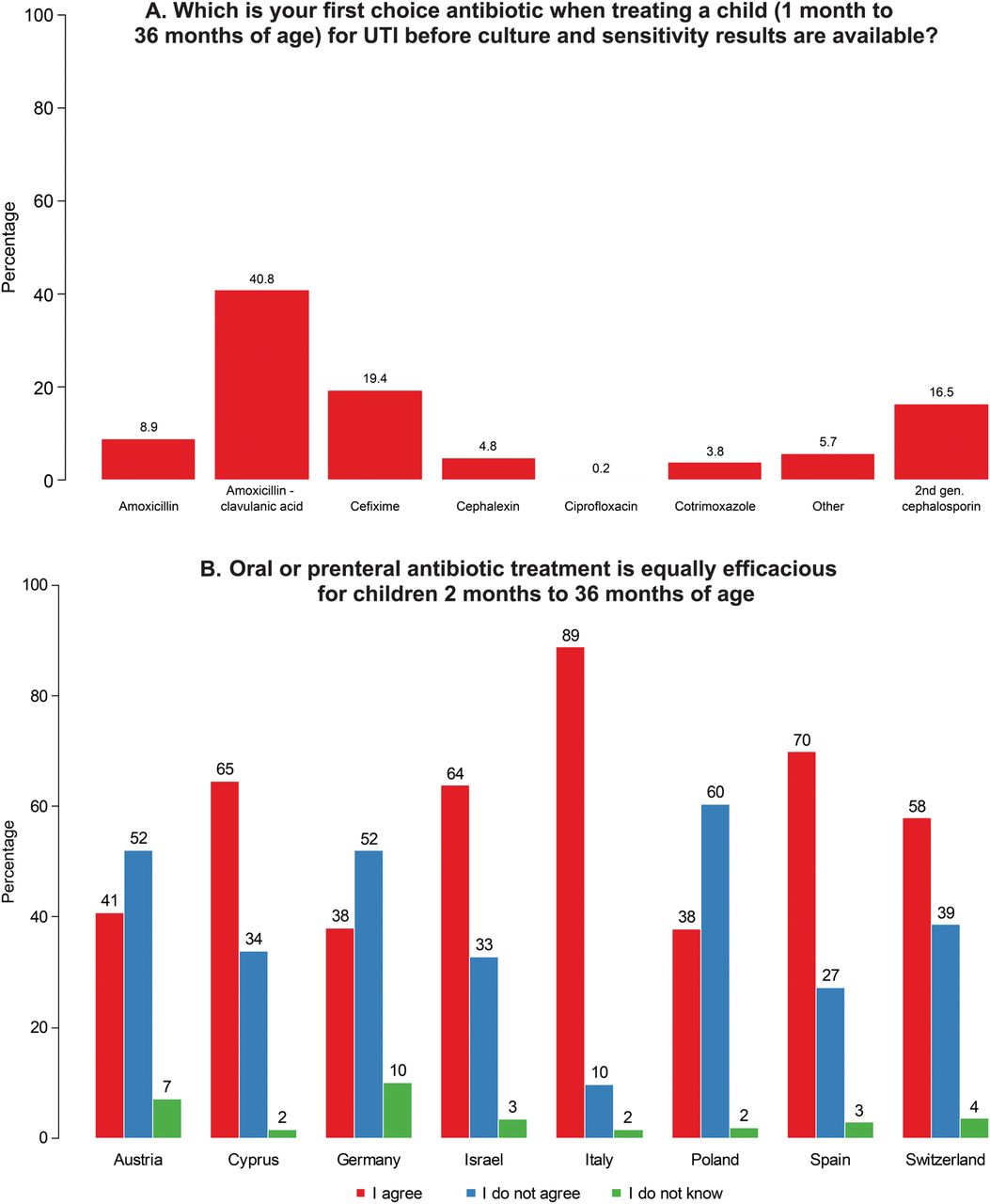
Antibiotic treatment of urinary tract infection (UTI). (A) Antibiotic preferences in Europe; (B) opinions on the efficacy of oral versus intravenous administration, data from the eight most representative countries.
Almost all of the participants (98%) treat a febrile UTI with a course of antibiotics lasting for 7–14 days. In the case of afebrile UTIs, children are treated for 3–5 days by 18% of respondents, for 7 days by 56% and for 10 days by 23%, with 1% prescribing either for 1–3 or 14 days.
Responders were presented with the following scenario: It's the weekend and laboratories are closed; you see a child, 1–36 months of age, with fever and suspected UTI. How would you proceed? Sixty-five per cent would start antibiotics after collecting urine to be stored in the fridge and sent for culture on Monday, 32% would start antibiotics immediately with no culture and 4% would wait until Monday to ask for culture and then start antibiotics.
Diagnostic work-up
A total of 947 respondents (84%) personally prescribe investigations and 245 of them (22%) perform the ultrasound evaluation themselves. Sixteen per cent refer the child to a paediatric nephrologist for diagnostic work-up and therefore were not required to answer questions regarding investigative procedures and prophylaxis.
Ultrasound
Eighty per cent of respondents prescribe ultrasound in all children aged 1–36 months, 7% in children aged <2 years and 13% in infants only.
Cystography
When asked if they recommend cystography in children with a confirmed diagnosis of UTI, 63% of the respondents said yes, but only if abnormalities are revealed during ultrasound evaluation. Twenty per cent ask for cystography in all children younger than 2 years, 12% only in infants and 5% in children of all ages.
Table 1 compares the recommendations of the three most recent guidelines. The different attitudes in Europe are shown in figure 3.

Prescription of cystography in different age groups. Data from the eight most representative countries.
VUR and prophylaxis
One out of four respondents recommends antibiotic prophylaxis for children with any grade of VUR, 39% for children with grades III–V and 24% for children with grades IV and V. Twelve per cent of the respondents do not prescribe prophylaxis for any grade of VUR (table 1). There are major differences among countries (figure 4). In table 1, the recommendations of the three most recent guidelines are compared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Prescription of antibiotic prophylaxis based on the presence and grade of reflux. Data from the eight most representative countries.
Data on urine collection, cystography prescription and antibiotic prophylaxis for the most representative countries are summarised in the tables available in the online supplementary appendix.
Discussion
Since 2000, six studies have been published evaluating the diagnosis and management of UTIs in primary care in the following countries: Belgium, Israel, The Netherlands, Ireland, the USA and Canada.17–22 These studies involved a small number of doctors in most cases and did not deal with all aspects of UTI diagnosis and management. In addition, three of the studies were surveys,18 ,19 ,22 one a clinical case review17 and two retrospective chart reviews.20 ,21
Therefore, we decided to obtain a more comprehensive view of European everyday clinical practice. There was a good response to our survey with 1129 paediatricians answering the questionnaire. The majority of respondents (91%) were primary care paediatricians working in the public sector. Our data show that most are actively involved in the diagnostic process, with 62% personally prescribing the diagnostic work-up and 22% performing ultrasound themselves.
Most paediatricians are well aware that UTI is a possible diagnosis in febrile children, with some focussing their attention mainly on the youngest patients (1–24 months of age). In fact, a recent meta-analysis reported that UTI is the cause of fever in 7% of febrile children with no other signs of infection.1 This meta-analysis also showed that uncircumcised boys <3 months of age have a much higher prevalence (20%) of UTI than circumcised boys (2.4%) of the same age. It is well known that not being circumcised is one of the most important clinical factors associated with UTIs, with an OR of 10.4 (95% CI 4.7–31.4).23 However, this fact does not seem to be well known, since only 50% of the participants in our survey agreed that not being circumcised is a risk factor for UTI.
Regarding UTI diagnosis and imaging work-up, it is clear that some decisions and characteristics are specific to certain countries. This may be because many different sets of guidelines have been published at local, national and international level, making it almost impossible for primary care paediatricians to adhere to the same set of guidelines. In addition, some of these guidelines are complicated to follow, long-winded and therefore difficult to remember.
Some of the differences revealed by the survey may be due to variations in national health systems and the different guideline recommendations for collecting urine. Use of urine collection bags predominates all over Europe, while suprapubic aspiration (SPA) is minimal (3.6%) even for very young infants. There are marked national differences, with Germany and Poland at the two extremes regarding the use of bags for children <3 months of age: a bag is used for the vast majority of urine collection in Germany, while the bag is not used at all for infants in Poland. Major differences were described in the surveys mentioned above: 80% of urine specimens were obtained by bag collection in Ireland,22 while 69% of urine specimens were obtained by catheterisation in 44 states in the USA.19
Although most guidelines agree that SPA or catheterisation is the most effective way to obtain uncontaminated urine samples for urine culture, there is a clear trend towards less invasive methods in clinical practice (table 1). Could this be due to non-compliance by the primary care paediatrician or to a lack of resources and the impracticability of certain procedures in the variety of routine clinical settings throughout Europe? It is fundamental when writing guidelines that they can be carried out easily and efficiently in the majority of settings where patients are treated.
Some other results from our questionnaire do not have a clear explanation. Why are there varying opinions regarding the efficacy of oral compared to intravenous antibiotics (60% agreed oral and intravenous antibiotics are equally efficacious, while 40% either disagreed or didn't know) with major differences being seen among countries? Why do 9% of our respondents prefer amoxicillin for the treatment of acute infection, when it is well known that it has a high resistance rate globally? Why do a substantial number of participants still prescribe cystography for all children? Why do some paediatricians continue to prescribe antibiotic prophylaxis for low-grade reflux?
While for controversial points it is understandable that there are different approaches at the country level, it is less acceptable that well-documented and proven approaches should be ignored. When well-constructed guidelines are published, there should be a concerted effort to implement them, also to reward the efforts that have been made to conduct the relevant studies and collect the necessary data. We should start thinking seriously about the educational strategies necessary to ensure the implementation of UTI guidelines. In this regard, a recent paper described a quality improvement implementation study aimed at achieving acceptance of AAP recommendations on when to perform a voiding cystourethrogram (VCUG) across multiple settings. The authors were able to achieve substantial adherence to the new recommendations in a short period of time (4 months).24 A further study showed a reduction in MCU requests and in prescriptions for antibiotic prophylaxis during the 2 years following publication of the NICE guidelines.25 These results are quite astounding and in contrast to our results, which are more in line with data reported in the literature indicating a much longer time for the implementation of guidelines.26
Strengths and weaknesses
The main strength of our study is the large number of respondents from a varying number of European countries. This provides a broader view of common practice.
The main weakness of our study is selection bias, caused by the voluntary nature of the survey and the fact that it is difficult to interpret the differences found in clinical practice as multiple sets of contradictory guidelines exist as do differences in national health systems. A limitation of secondary importance is that this survey mainly reflects the attitude of paediatricians towards children with non-complicated UTIs, as complicated cases are generally seen in a hospital setting.
In conclusion, our survey shows marked heterogeneity among European countries regarding the diagnosis and management of febrile UTIs. Moreover, numerous discrepancies between best practice guidelines and reality are evident. This highlights the need for the development of simple, short, practical and easy-to-remember guidelines and of educational strategies to ensure their implementation.
Acknowledgments
The authors wish to thank the EAPRASnet coordinators for their dedication and commitment. Without their effort and enthusiasm, this research project would not have been completed. We also want to express gratitude to all EAPRASnet members who have participated in our common endeavours and were willing to share their invaluable experience and their precious time. We are profoundly indebted to Lena Group for their invaluable technical support and for their extended and professional assistance in data collection and reporting.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online tables
Footnotes
-
Contributors All authors were involved in developing the questionnaire and revising the manuscript. AH and GM wrote the manuscript. GM is guarantor.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.