Article Text

Abstract
Objectives: To investigate the numbers and types of joint and soft tissue injections performed by general practitioners (GPs) and to explore attitudes to training in joint and soft tissue injection and perceived barriers to performing injections.
Methods: A self administered questionnaire was mailed to a random sample of 410 (30%) of 1367 GPs in Northern Ireland. Two mailings were used to increase the response rate. Questions explored the GPs’ demographic characteristics, types and numbers of injections performed, previous training experience, attitudes towards training, and perceived barriers.
Results: The overall response rate was 75%. Practitioners who were men, worked in a “rural” or “mixed” locality, and had had a previous post in rheumatology, orthopaedics, or sports medicine were more likely to perform joint and soft tissue injections. Forty six per cent of GPs did not currently perform any injections; 5% of GPs performed most of the injections in the community. Injections into the shoulder, knee, and lateral epicondylitis were found to be the most commonly performed injections. The GPs preferred to train on “real patients” rather than “mannequin models”. Those GPs who had trained on “real patients” were more likely to perform injections. The main perceived barrier to performing joint and soft tissue injections in the community was the “inability to maintain injection skills”.
Conclusion: Postgraduate training, methods of training, and the ability to maintain injection skills seemed to be determinants affecting GP confidence and the amount of joint and soft tissue injections that they performed. Most injections were performed by a few GPs in the community. These findings may have implications for the developing role of GP specialists in primary care trusts.
- intra-articular injections
- soft tissue injection
- training
- general practitioner
- 95% CI, 95% confidence interval
- GP, general practitioner
Statistics from Altmetric.com
Musculoskeletal disorders are a common reason for consultation with a general practitioner (GP).1 Such disorders represent a significant cause of disability and morbidity.2–4 For many of these disorders, treatment with corticosteroid injections can bring about a rapid and effective response with a very low complication rate.5–9
In Northern Ireland, as with the rest of the United Kingdom, the 1990 contract encouraged GP principals to perform minor surgical procedures, including joint and soft tissue injections, in the community. To attract payments for procedures, GPs had to undertake recognised training, which would make them eligible for inclusion on the minor surgery list. Minor surgical procedures performed by GPs have been shown to be cost effective and popular with patients.10 However, many GPs are reluctant to perform joint and soft tissue injections and continue to refer their patients to hospital. In 1990, when renumeration for GP principals performing minor surgery was introduced, rheumatologists expressed their support, thinking that rheumatology waiting lists would be reduced.11 Despite the increased fees paid to GPs, there has been no reduction in hospital referrals.12
We are aware that there is a need for improvement in rheumatology education during GP vocational training and that GPs lack confidence in managing musculoskeletal problems.13 Vocational training for GPs, primary care structure, and access to secondary care in Northern Ireland, are similar to the rest of the United Kingdom. To date there is little information about the types of injections performed in the community or GPs’ reasons for not providing this service. The aims of this paper were to ascertain the numbers and types of injections performed, perceived barriers to performing injections, and attitudes towards various methods of training in joint and soft tissue injection skills.
METHODS
A self administered questionnaire was developed from a focus group of GPs. The focus group comprised men and women from rural, urban, and mixed practices, and included principal and non-principal GPs. The focus group was purposely selected for its heterogeneity to capture differences in opinions and experiences.
The questionnaire aimed to (a) quantify the number and different types of injections performed by GPs in the past year; (b) to evaluate the level of training and how GPs thought that this training improved their ability and confidence to perform injections. Levels of confidence were measured on a five point Likert scale with response options from “strongly agree” to “strongly disagree”; and (c) to identify barriers to GPs performing joint and soft tissue injections in the community. Responses were measured on a five point Likert scale with options varying form “very likely” to “very unlikely”.
A convenient sample of GPs was chosen to pilot the questionnaire. The revised questionnaire was mailed to a random sample of 410 of 1367 (30%) GPs in Northern Ireland. A single reminder was sent to non-responders after four weeks and returned questionnaires were analysed after 10 weeks. Questionnaires were numerically coded to ensure confidentiality and the study was approved by the Queen’s University of Belfast research ethics committee (application No 85/01). Logistic regression was used to determine the likelihood of respondents performing injections by their demographic characteristics.
RESULTS
Response rate
A total of 310 of 410 questionnaires were returned (76% response rate). One questionnaire was incomplete and was not used in the analysis.
Demographic characteristics of respondents
Table 1 outlines the demographic characteristics of the sample and whether or not the respondents had performed joint and soft tissue injections in the last year.
Demographic characteristics of respondents
Logistic regression analysis showed that male GPs, GPs who classified themselves as working in a “rural” or “mixed” locality, and GPs who had received formal training in performing joint and soft tissue injections, in a postgraduate post (for example, rheumatology, orthopaedics, or sports medicine), were more likely to perform injections (table 2). Of the 246 GP principals, 196 (80%) were on the minor surgery list. Those GPs who were on the list were significantly more likely to perform injections (table 2).
Logistic regression analysis of the likelihood of GPs performing joint/soft tissue injections by their demographic characteristics
Joint and soft tissue injection activity
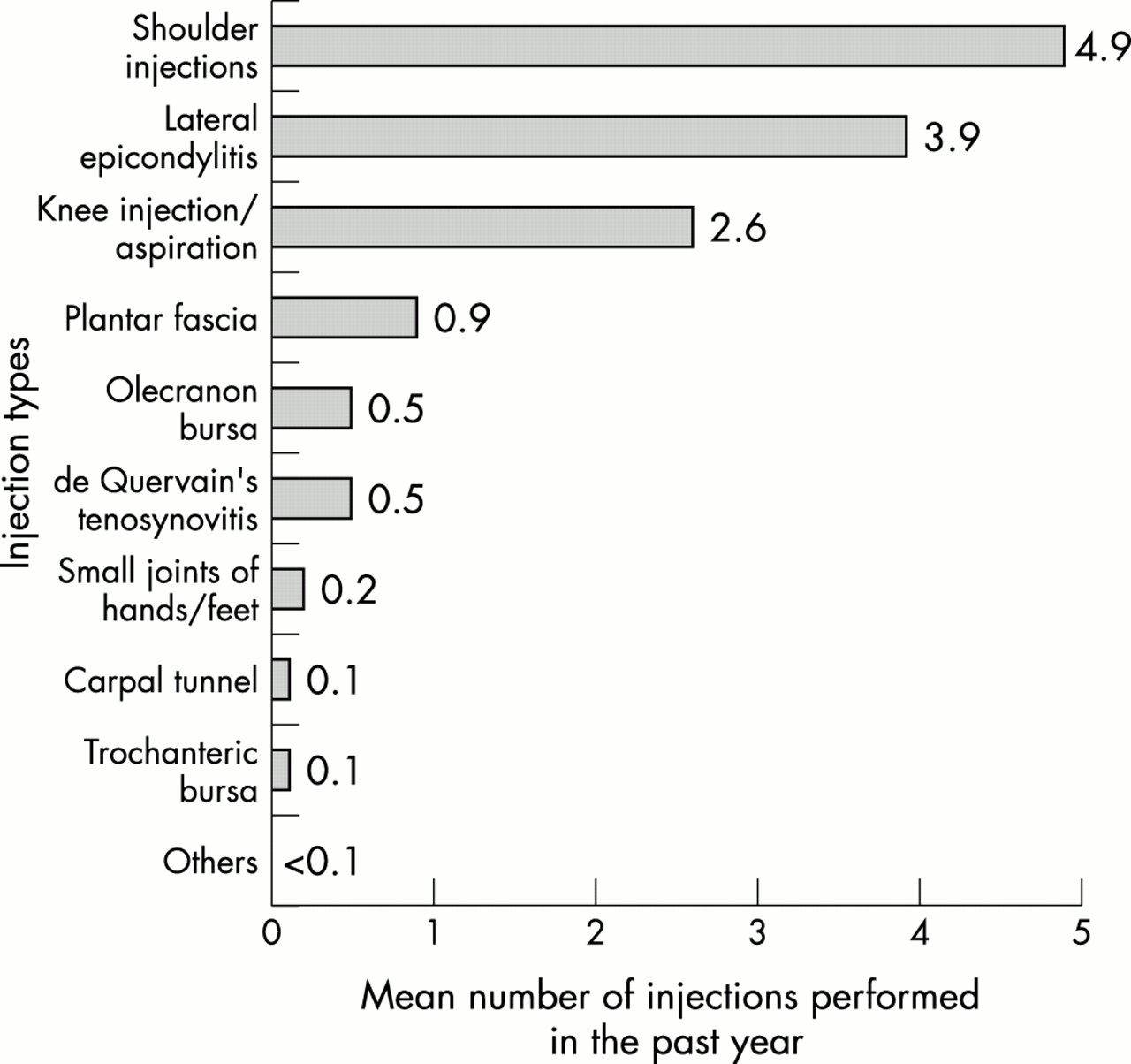
Over half (54%; 166/309) of the respondents stated that they had performed joint and soft tissue injection(s) within the past year. Interestingly, 5% (16/309) of respondents performed most (51%; 2094/4072) of the injections. The most common types of injections performed were shoulder injections, followed by lateral epicondylitis injections and knee injections and aspirations (fig 1).
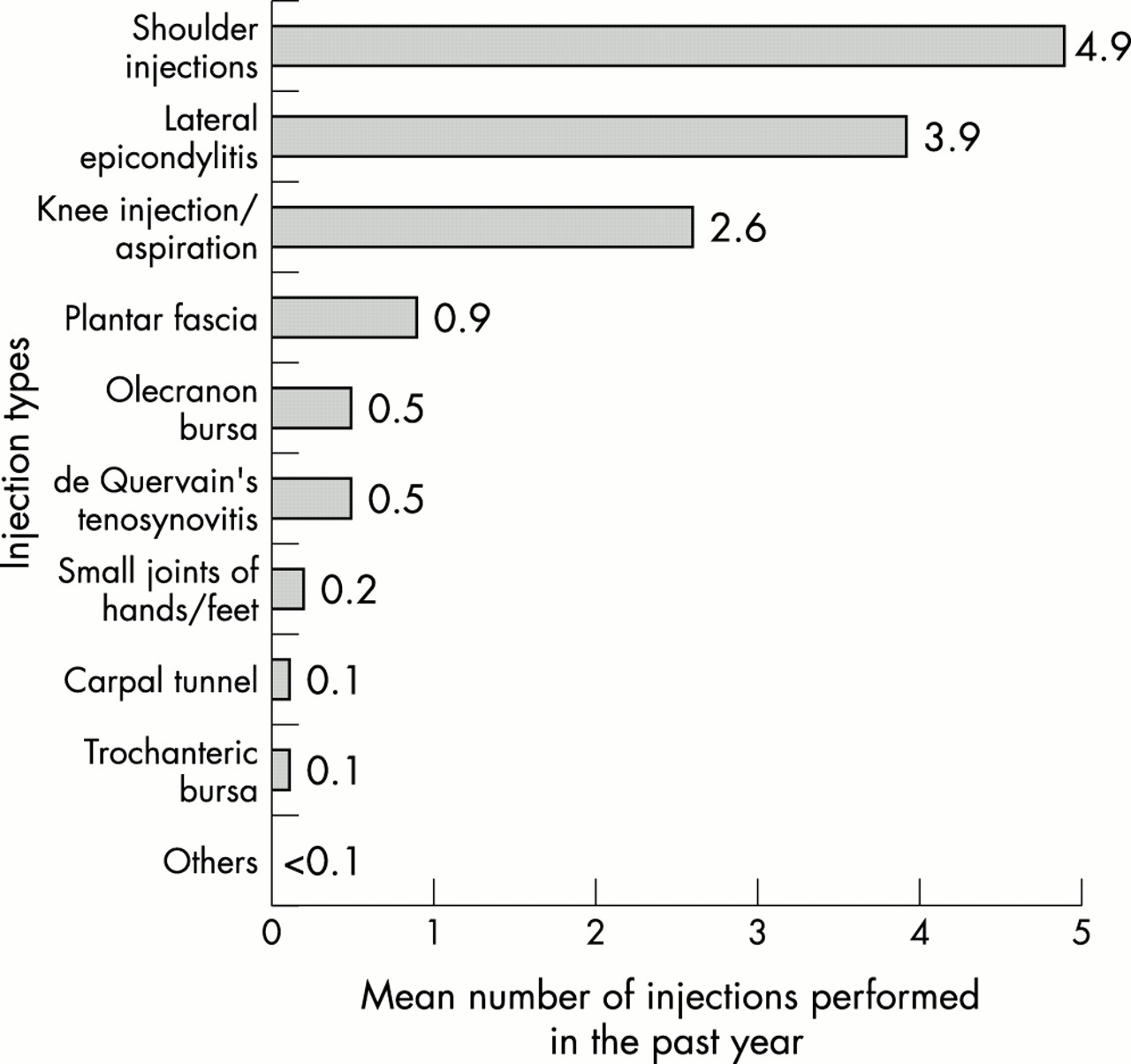
Numbers and types of joint and soft tissue injections performed by respondents in the past year.
In response to the question “have you ever performed joint and soft tissue injections in your career”, of the GPs who no longer performed injections, 83% (118/143) had previously carried out an injection at some stage in their career.
Joint and soft tissue injection training
Sixty seven per cent (206/309) of respondents stated that they had been to a training course in the past five years. Of these 206 respondents, 76 (37%) had not performed any injections within the previous year.
The GPs were asked if they had ever attended a training course using either a “mannequin model” or “real patients”; 226 of 309 (73%) respondents stated that they had attended a training course using mannequin models and only 29 of 309 (9%) respondents had been to a course where they trained on real patients.
The GPs were also asked how they perceived the effect of these training methods on their “confidence and ability to perform joint and soft tissue injections”. Respondents who received training on real patients were significantly more confident in performing injections than respondents who trained using mannequin models (t=4.20; 22 df; p<0.001). Logistic analysis showed that GPs who trained on real patients were significantly more likely to have performed injections within the past year (χ2 =5.41, 1 df; p=0.02).
Perceived barriers to performing joint and soft tissue injections
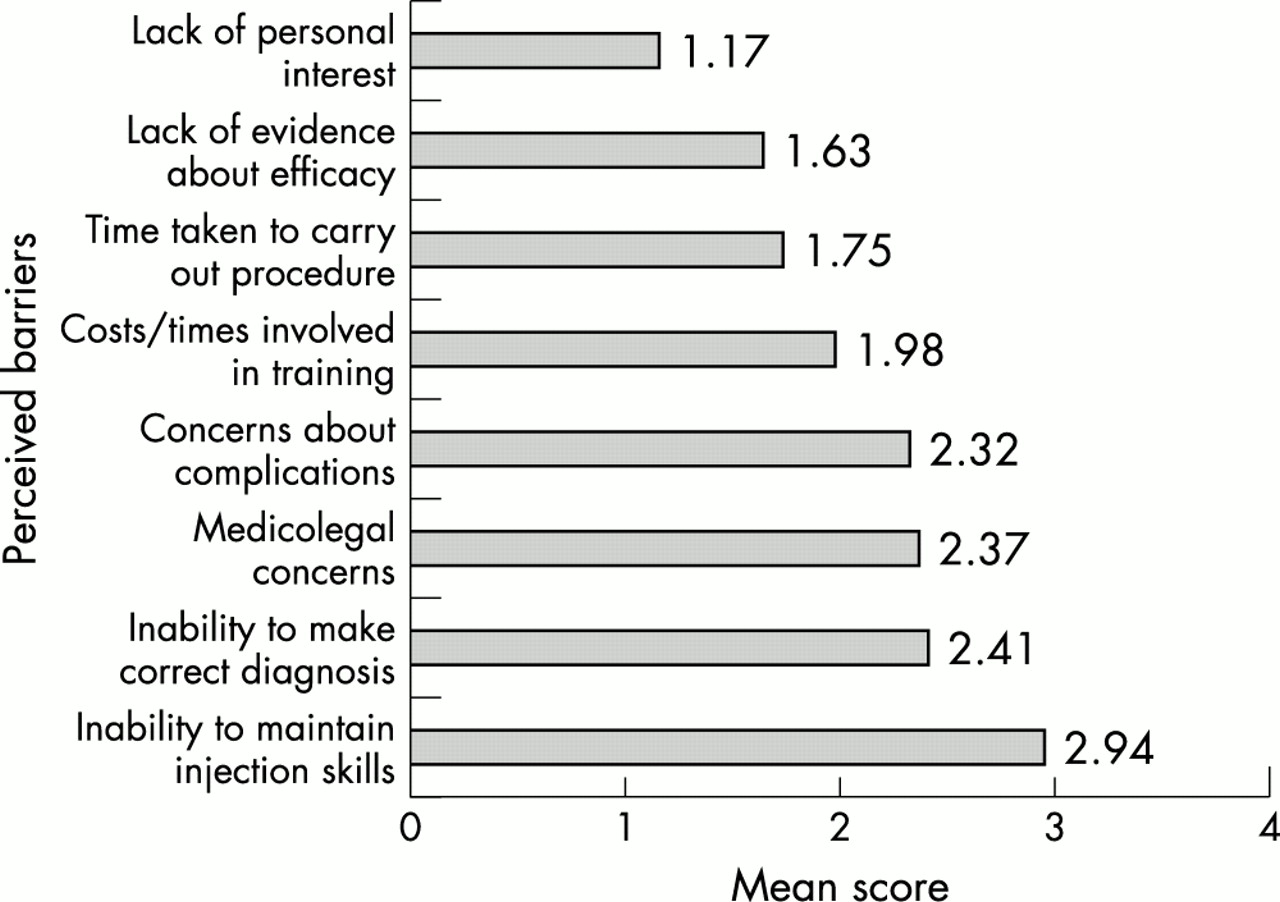
The main perceived barrier to performing joint and soft tissue injections was “Inability to maintain injection skills” (fig 2). This was followed by a lack of confidence among GPs in making the “correct clinical diagnosis”. The GPs were also concerned about “complications” and “medicolegal” issues. Most respondents did not perceive “lack of personal interest, lack of evidence about the efficacy of injections, time taken to perform procedures, and time and costs of training” as barriers.
{kind=link}
{kind=link}
Perceived levels of barriers to performing joint and soft tissue injections in the community.
DISCUSSION
Our results show that GPs who were men, were included on the minor surgery list, and worked in a “rural” or “mixed” locality were more likely to perform joint and soft tissue injections. Those who had received formal training in joint and soft tissue injection in a previous postgraduate post, such as rheumatology, sports medicine, or orthopaedics, were found to be more likely to perform injections—but as our results show, only a few respondents had been in such posts.
In an initiative by the Arthritis Research Campaign, Primary Care Rheumatology Society, and the Royal College of General Practitioners, a curriculum was proposed for GPs and GP registrars in the United Kingdom.14 The consensus view of this group was that joint and soft tissue injections should not be a core skill for all GPs. Given that most injections are performed by only a few GPs in the community, perhaps the training of all GPs to perform joint and soft tissue injections is an unattainable goal. Given the developing role of GP specialists in primary care trusts, in which rheumatology has been identified as a key area, there is a need to focus joint and soft tissue injection training on these doctors.15
Training on mannequin models was the most commonly cited teaching method for training in joint and soft tissue injection, but over a third of GPs (37%) who had been on such courses, had not performed any injections within the past year. Logistic regression analysis confirmed that GPs who received training on real patients were more likely to perform injections. Availability (only 9% of respondents had attended “real patient” courses) was a limiting factor.
The goal of any skill training should be a change in the behaviour of the learner and repeated practice should enhance the retention of those skills. It was interesting to note that respondents perceived “an inability to maintain injection skills” as the main barrier to performing injections. This is supported by the finding that 83% of GPs who no longer performed injections, had previously done so at some stage in their career. If GPs were helped to maintain their injections skills (regular refresher training sessions at hospital injection clinics; opportunities to specialise within primary care groups) the numbers of patients injected in the community may increase. Given that shoulder, knee, and lateral epicondyle injections were the most commonly performed, any training programme should concentrate on these types of injections. There was a desire among GPs for courses to include training on diagnosis and medicolegal concerns.
The GPs who are on the minor surgery list can claim fees for performing 15 minor surgery cases every three months.16 This system of remuneration is unfavourable to the small percentage (5%) of GPs who perform most of the injections in the community. We also found that over a third (37%) of respondents on the minor surgery list had not performed any injections within the past year.
The aim of our study was to assess GPs’ attitudes and experiences in training and performing joint and soft tissue injections in the community. We were gratified by the high response rate but given that the questionnaire responses were anonymous, we were unable to assess the characteristics of non-respondents. The responses to the survey were not validated with GP records. Confidence, as measured in this study, may relate to the concept of perceived self efficacy, which does not automatically translate into clinical competence.
In conclusion, GPs exhibit a wide variety of experiences and attitudes towards performing joint and soft tissue injections in the community. Postgraduate training, methods of training, and the ability to maintain injection skills seem to be determinants of GP confidence in numbers of injections they perform. At present it seems that a few GPs perform most injections in the community. It may be that the efforts of rheumatologists should be focused on the training of GP specialists with a particular interest in rheumatology who wish to develop their injection skills further.
Acknowledgments
We are grateful to the Stone Forum for financial support.