Long-Term Risk Factor Control After Myocardial Infarction—A Need for Better Prevention Programmes

 ,
,
Abstract
:1. Introduction: Long-Term Prognosis after Myocardial Infarction
2. “Real World“ Data on Long-Term RFC in Patients after MI
3. Preventive Strategies
4. Discussion: How to Improve Long-Term Risk Factor Control?
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
List of Abbreviations
| BSR | Bremen STEMI-registry |
| CAD | Coronary artery disease |
| CANTOS | Canakinumab anti-inflammatory thrombosis outcomes study |
| COURAGE | Clinical outcomes utilizing revascularization and aggressive drug evaluation |
| DYSIS | Dyslipidemia international study |
| EUROASPIRE | European action on secondary and primary prevention by intervention to reduce events |
| hsCRP | High-sensitivity C-reactive protein |
| IPAQ | International physical activity questionnaire |
| IPP | Intensive prevention programme |
| MACCE | Major adverse cardiac and cerebrovascular events (death, infarction, stroke) |
| MI | Myocardial infarction |
| OASIS 5 | Organization to assess strategies in acute ischemic syndromes 5 |
| OPTICARE | Optimal cardiac rehabilitation |
| RESPONSE II | Randomized evaluation of secondary prevention by outpatient nurse specialists II |
| RFC | Risk factor control |
| STEMI | ST-segment elevation myocardial infarction |
| SYNTAX | Synergy between PCI with TAXUS drug-eluting stent and cardiac surgery |
| UC | Usual care |
References
- Yeh, R.W.; Sidney, S.; Chandra, M.; Sorel, M.; Selby, J.V.; Go, A.S. Population trends in the incidence and outcomes of acute myocardial infarction. N. Engl. J. Med. 2010, 362, 2155–2165. [Google Scholar] [CrossRef] [PubMed]
- Jernberg, T.; Hasvold, P.; Henriksson, M.; Hjelm, H.; Thuresson, M.; Janzon, M. Cardiovascular risk in post-myocardial infarction patients: Nationwide real world data demonstrate the importance of a long-term perspective. Eur. Heart J. 2015, 36, 1163–1170. [Google Scholar] [CrossRef] [PubMed]
- Backhaus, T.; Fach, A.; Schmucker, J.; Fiehn, E.; Garstka, D.; Stehmeier, J.; Hambrecht, R.; Wienbergen, H. Management and predictors of outcome in unselected patients with cardiogenic shock complicating acute ST-segment elevation myocardial infarction: Results from the Bremen STEMI Registry. Clin. Res. Cardiol. 2018, 107, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Kudaibergenov, A.; Wienbergen, H.; Fach, A.; Schmucker, J.; Garstka, D.; Hamann, J.; Backhaus, T.; Osteresch, R.; Hambrecht, R. 5-year-outcomes after STEMI—Which patients have the best long-term course? Clin. Res. Cardiol. 2018, 107, V1329. [Google Scholar]
- Thiele, H.; Ohman, E.M.; Desch, S.; Eitel, I.; de Waha, S. Management of cardiogenic shock. Eur. Heart J. 2015, 36, 1223–1230. [Google Scholar] [CrossRef] [Green Version]
- Chow, C.K.; Jolly, S.; Rao-Melacini, P.; Fox, K.A.; Anand, S.S.; Yusuf, S. Association of diet, exercise, and smoking modification with risk of early cardiovascular events after acute coronary syndromes. Circulation 2010, 121, 750–758. [Google Scholar] [CrossRef] [PubMed]
- Maron, D.J.; Mancini, G.B.J.; Hartigan, P.M.; Spertus, J.A.; Sedlis, S.P.; Kostuk, W.J.; Berman, D.S.; Teo, K.K.; Weintraub, W.S.; Boden, W.E. Healthy Behavior, Risk Factor Control, and Survival in the COURAGE Trial. J. Am. Coll. Cardiol. 2018, 72, 2297–2305. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corra, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovasular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar]
- Shah, N.D.; Dunlay, S.M.; Ting, H.H.; Montori, V.M.; Thomas, R.J.; Wagie, A.E.; Roger, V.L. Long-term medication adherence after myocardial infarction: Experience of a community. Am. J. Med. 2009, 122, 961.e7–961.e13. [Google Scholar] [CrossRef]
- Mangiapane, S.; Busse, R. Prescription prevalence and continuing medication use for secondary prevention after myocardial infarction: The reality of care revealed by claims data analysis. Dtsch. Aerztebl. Int. 2011, 108, 856–862. [Google Scholar]
- Kotseva, K. The EUROASPIRE surveys: Lessons learned in cardiovascular disease prevention. Cardiovasc. Diagn. Ther. 2017, 7, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Kotseva, K.; De Backer, G.; De Bacquer, D.; Ryden, L.; Hoes, A.; Grobee, D.; Maggioni, A.; Marques-Vidal, P.; Jennings, C.; Abreu, A.; et al. Lifestyle and impact on cardiovascular risk factor control in coronary patients across 27 countries: Results from the European Society of Cardiology ESC-EORP EUROASPIRE V registry. Eur. J. Prev. Cardiol. 2019, 26, 824–835. [Google Scholar] [CrossRef] [PubMed]
- Gitt, A.K.; Lautsch, D.; Ferrieres, J.; De Ferrari, G.M.; Vyas, A.; Baxter, C.A.; Bash, L.D.; Ashton, V.; Horack, M.; Almahmeed, W.; et al. Cholesterol target value attainment and lipid-lowering therapy in patients with stable or acute coronary heart disease: Results from the Dyslipidemia International Study II. Atherosclerosis 2017, 266, 158–166. [Google Scholar] [CrossRef] [PubMed]
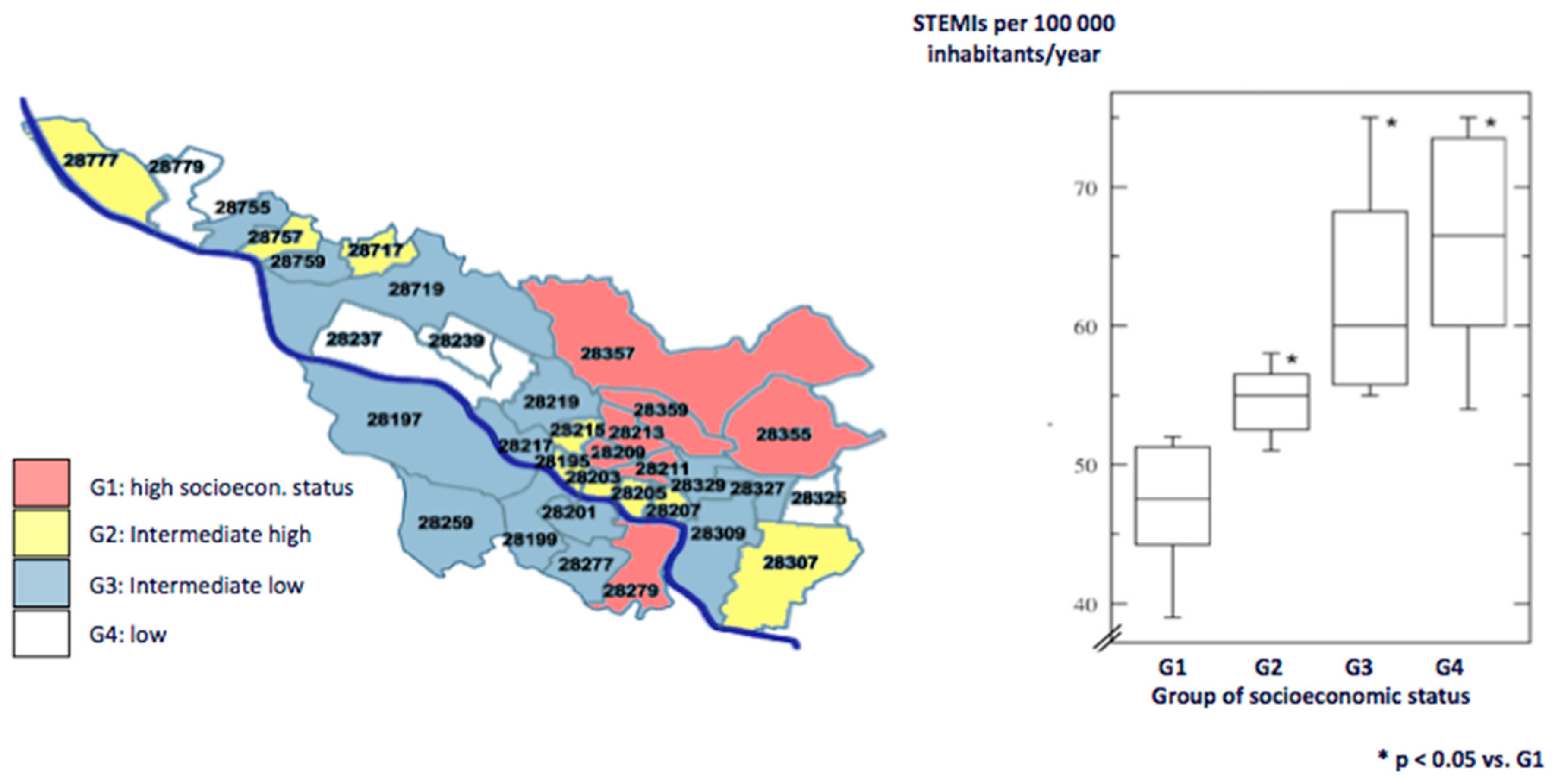
- Schmucker, J.; Seide, S.; Wienbergen, H.; Stehmeier, J.; Guenther, K.; Ahrens, W.; Hambrecht, R.; Pohlabeln, H.; Fach, A. Socially disadvantaged city districts show a higher incidence of acute ST-elevation myocardial infarctions with elevated cardiovascular risk factors and worse prognosis. BMC Cardiovasc. Dis. 2017, 17, 254. [Google Scholar] [CrossRef] [PubMed]
- Wienbergen, H.; Backhaus, T.; Mata Marin, L.; Fach, A.; Buenger, S.; Stehmeier, J.; Garstka, D.; Michel, S.; Kraemer, K.; Hambrecht, R. Young patients after ST-segment elevation myocardial infarction in clinical practice: Is secondary prevention as good as it should be? Eur. J. Prev. Cardiol. 2017, 24, 180. [Google Scholar]
- Kuepper-Nybelen, J.; Rothenbacher, D.; Hahmann, H.; Wusten, B.; Brenner, H. Changes of risk factors in patients with coronary heart disease after in-patient rehabilitation. Dtsch. Med. Wochenschr. 2003, 128, 1525–1530. [Google Scholar]
- Giannuzzi, P.; Temporelli, P.L.; Marchioli, R.; Maggioni, A.P.; Balestroni, G.; Ceci, V.; Chieffo, C.; Gattone, M.; Griffo, R.; Schweiger, C.; et al. Global secondary prevention strategies to limit event recurrence after myocardial infarction: Results of the GOSPEL study, a multicenter, randomized controlled trial from the Italian Cardiac Rehabilitation Network. Arch. Intern. Med. 2008, 168, 2194–2204. [Google Scholar] [CrossRef]
- Wood, D.A.; Kotseva, K.; Connolly, S.; Jennings, C.; Mead, A.; Jones, J.; Holden, A.; De Bacquer, D.; Collier, T.; De Backer, G.; et al. Nurse-coordinated multidisciplinary, family-based cardiovascular disease prevention programme (EUROACTION) for patients with coronary heart disease and asymptomatic individuals at high risk of cardiovascular disease: A paired, cluster-randomised controlled trial. Lancet 2008, 371, 1999–2012. [Google Scholar]
- Jorstad, H.T.; von Birgelen, C.; Alings, A.M.; Liem, A.; van Dantzig, J.M.; Jaarsma, W.; Lok, D.J.; Kragten, H.J.; de Vries, K.; de Miliano, P.A.; et al. Effect of a nurse-coordinated prevention programme on cardiovascular risk after an acute coronary syndrome: Main results of the RESPONSE randomised trial. Heart 2013, 99, 1421–1430. [Google Scholar] [CrossRef]
- Mayer-Berger, W.; Simic, D.; Mahmoodzad, J.; Burtscher, R.; Kohlmeyer, M.; Schwitalla, B.; Redaelli, M. Efficacy of a long-term secondary prevention programme following inpatient cardiovascular rehabilitation on risk and health-related quality of life in a low-education cohort: A randomized controlled study. Eur. J. Prev. Cardiol. 2014, 21, 145–152. [Google Scholar] [CrossRef]
- Sunamura, M.; Ter Hoeve, N.; van den Berg-Emons, H.J.; Haverkamp, M.; Redekop, K.; Geleijnse, M.L.; Stam, H.J.; Boersma, E.; van Domburg, R.T. OPTImal CArdiac REhabilitation (OPTICARE) following Acute Coronary Syndromes: Rationale and design of a randomised, controlled trial to investigate the benefits of expanded educational and behavioural intervention programs. Neth. Heart J. 2013, 21, 324–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sunamura, M.; Ter Hoeve, N.; van den Berg-Emons, R.J.G.; Geleijnse, M.L.; Haverkamp, M.; Stam, H.J.; Boersma, E.; van Domburg, R.T. Randomised controlled trial of two advanced and extended cardiac rehabilitation programmes. Heart 2018, 104, 430–437. [Google Scholar] [CrossRef] [PubMed]
- Minneboo, M.; Lachman, S.; Snaterse, M.; Jorstad, H.T.; Ter Riet, G.; Boekholdt, S.M.; Scholte Op Reimer, W.J.M.; Peters, R.J.G. Community-Based Lifestyle Intervention in Patients With Coronary Artery Disease: The RESPONSE-2 Trial. J. Am. Coll. Cardiol. 2017, 70, 318–327. [Google Scholar] [CrossRef] [PubMed]
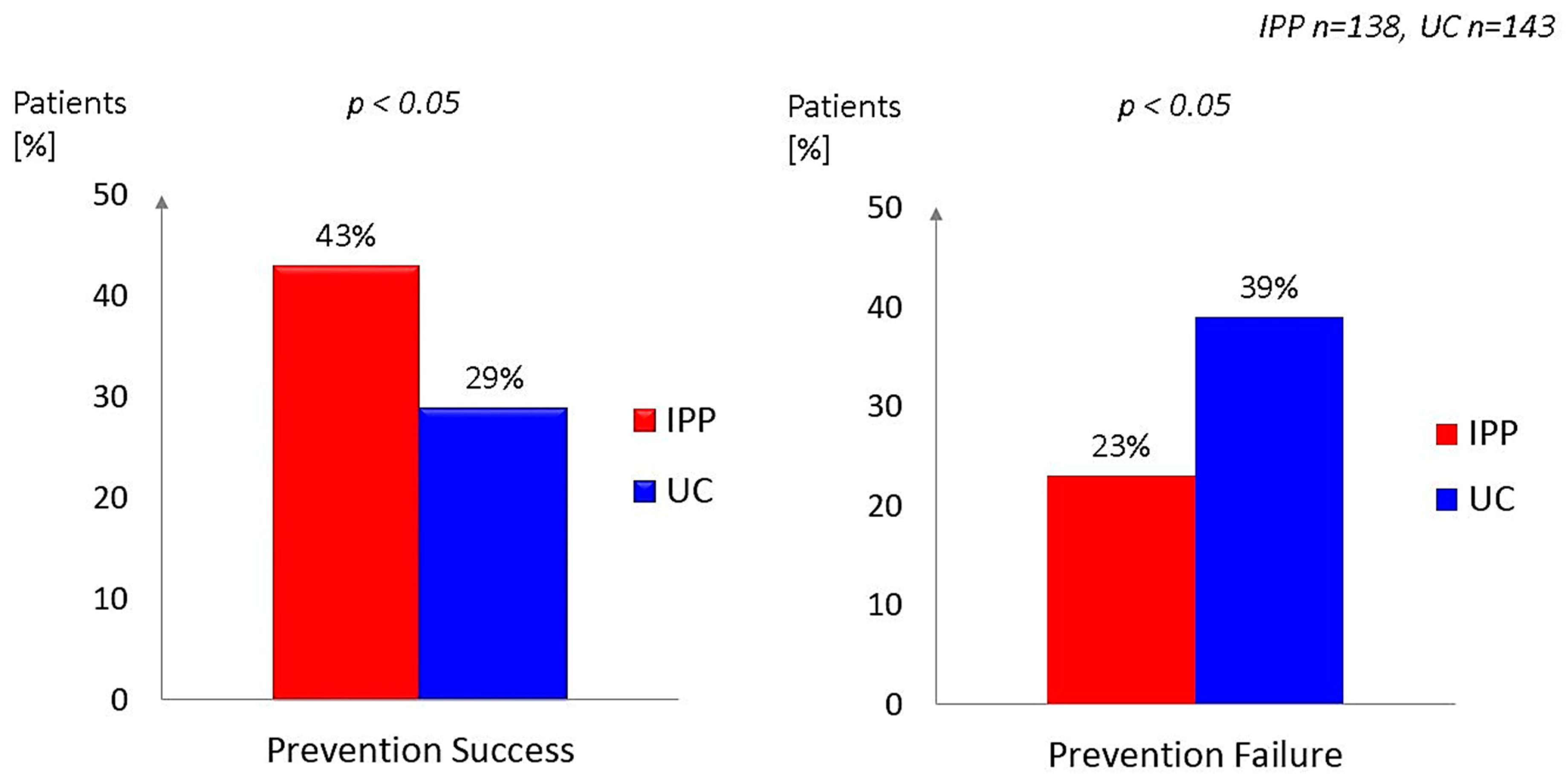
- Wienbergen, H.; Fach, A.; Meyer, S.; Meyer, J.; Stehmeier, J.; Backhaus, T.; Michel, S.; Kraemer, K.; Osteresch, R.; Schmucker, J.; et al. Effects of an intensive long-term prevention programme after myocardial infarction—A randomized trial. Eur. J. Prev. Cardiol. 2019, 26, 522–530. [Google Scholar] [CrossRef] [PubMed]
- Wienbergen, H.; Backhaus, T.; Michel, S.; Stehmeier, J.; Kraemer, K.; Schmucker, J.; Meyer, S.; Meyer, J.; Haase, H.; Elsaesser, A.; et al. Assessment and control of physical activity by step counters and online documentation in secondary prevention after myocardial infarction. Eur. Heart J. 2017, 38, P2476. [Google Scholar] [CrossRef]
- Backhaus, T.; Meyer, S.; Meyer, J.; Fach, A.; Schmucker, J.; Osteresch, R.; Stehmeier, J.; Wettwer, T.; Haase, H.; Elsaesser, A.; et al. Which role plays school degree in effectiveness of prevention after myocardial infarction? Eur. Heart J. 2018, 39, P1228. [Google Scholar] [CrossRef]
- Gueder, G.; Stoerk, S.; Gelbrich, G.; Brenner, S.; Deubner, N.; Morbach, C.; Wallenborn, J.; Berliner, D.; Ertl, G.; Angermann, C.E. Nurse-coordinated collaborative disease management improves the quality of guideline-recommended heart failure therapy, patient-reported outcomes, and left ventricular remodelling. Eur. J. Heart Fail. 2015, 17, 442–452. [Google Scholar] [CrossRef] [Green Version]
- Mega, J.L.; Stitziel, N.O.; Smith, J.G.; Chasman, D.I.; Caulfield, M.J.; Devlin, J.J.; Nordio, F.; Hyde, C.L.; Cannon, C.P.; Sacks, F.M.; et al. Genetic risk, coronary heart disease events, and the clinical benefit of statin therapy: An analysis of primary and secondary prevention trials. Lancet 2015, 385, 2264–2271. [Google Scholar] [CrossRef]
- Kullo, I.J.; Jouni, H.; Austin, E.E.; Brown, S.A.; Kruisselbrink, T.M.; Isseh, I.N.; Haddad, R.A.; Marroush, T.S.; Shameer, K.; Olson, J.E.; et al. Incorporating a Genetic Risk Score Into Coronary Heart Disease Risk Estimates: Effect on Low-Density Lipoprotein Cholesterol Levels (the MI-GENES Clinical Trial). Circulation 2016, 133, 1181–1188. [Google Scholar] [CrossRef]
- Williams, M.S. Early Lessons from the Implementation of Genomic Medicine Programs. Annu. Rev. Genom. Hum. Genet. 2019. [Google Scholar] [CrossRef]
- Ridker, P.M.; MacFadyen, J.G.; Everett, B.M.; Libby, P.; Thuren, T.; Glynn, R.J. Relationship of C-reactive protein reduction to cardiovascular event reduction following treatment with canakinumab: A secondary analysis from the CANTOS randomised controlled trial. Lancet 2018, 391, 319–328. [Google Scholar] [CrossRef]
- Gielen, S.; Adams, V.; Moebius-Winkler, S.; Linke, A.; Erbs, S.; Yu, J.; Kempf, W.; Schubert, A.; Schuler, G.; Hambrecht, R. Anti-inflammatory effects of exercise training in the skeletal muscle of patients with chronic heart failure. J. Am. Coll. Cardiol. 2003, 42, 861–868. [Google Scholar] [CrossRef]
- Walther, C.; Moebius-Winkler, S.; Linke, A.; Bruegel, M.; Thiery, J.; Schuler, G.; Hambrecht, R. Regular exercise training compared with percutaneous intervention leads to a reduction of inflammatory markers and cardiovascular events in patients with coronary artery disease. Eur. J. Cardiovasc. Prev. Rehabil. 2008, 15, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Zhernakova, D.V.; Le, T.H.; Kurilshikov, A.; Atanasovska, B.; Bonder, M.J.; Sanna, S.; Claringbould, A.; Vosa, U.; Deelen, P. Individual variations in cardiovascular-disease-related protein levels are driven by genetics and gut microbiome. Nat. Genet. 2018, 50, 1524–1532. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.H.W.; Baeckhed, F.; Landmesser, U.; Hazen, S.L. Intestinal Microbiota in Cardiovascular Health and Disease: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 73, 2089–2105. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Prevention success Improvement of one risk factor without deterioration of another Prevention failure Deterioration of one risk factor without improvement of another | ||
| Risk factors | Improvement | Deterioration |
| Smoking | Smoking cessation (at least for 4 weeks at evaluation, controlled by serum cotinine levels) | New or recurrent active smoking |
| LDL cholesterol | Reduction < 5 mg/dL | Increase ≥ 5 mg/dL |
| Physical inactivity | Increase of caloric expenditure ≥ 500 kcal/week (leisure time moderate or vigorous physical activity assessed by IPAQ) | Decrease of caloric expenditure ≥ 500 kcal/week |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Osteresch, R.; Fach, A.; Schmucker, J.; Eitel, I.; Langer, H.; Hambrecht, R.; Wienbergen, H. Long-Term Risk Factor Control After Myocardial Infarction—A Need for Better Prevention Programmes. J. Clin. Med. 2019, 8, 1114. https://doi.org/10.3390/jcm8081114
Osteresch R, Fach A, Schmucker J, Eitel I, Langer H, Hambrecht R, Wienbergen H. Long-Term Risk Factor Control After Myocardial Infarction—A Need for Better Prevention Programmes. Journal of Clinical Medicine. 2019; 8(8):1114. https://doi.org/10.3390/jcm8081114
Chicago/Turabian StyleOsteresch, Rico, Andreas Fach, Johannes Schmucker, Ingo Eitel, Harald Langer, Rainer Hambrecht, and Harm Wienbergen. 2019. "Long-Term Risk Factor Control After Myocardial Infarction—A Need for Better Prevention Programmes" Journal of Clinical Medicine 8, no. 8: 1114. https://doi.org/10.3390/jcm8081114