
Abstract
Background
Many studies focus on interventions that reduce the processes that lead to adverse drug events (ADEs), such as inappropriate or high-risk prescribing, without assessing whether they result in a reduction in ADEs or associated adverse health outcomes.
Objectives
Our objective was to systematically review interventions to reduce the incidence of ADEs measured by health outcomes in older patients in primary care settings.
Methods
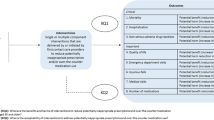
The review included randomised controlled trials, controlled clinical trials, controlled before and after studies, interrupted time series studies and cohort studies conducted in the community care setting. Older patients (aged ≥ 65 years) receiving medical treatment in primary care were included. Interventions were aimed at reducing adverse health outcomes associated with ADEs in older patients. Risk of bias was assessed using the Cochrane Collaboration’s tool. Outcomes were measured by reductions in hospitalisation, emergency department (ED) visits, mortality and improvements in quality of life (QoL), mental health and physical function. Fixed and random-effects models were used to calculate pooled effect estimates comparing interventions and control groups for the outcomes, where feasible.
Results
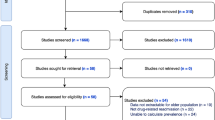
The literature search identified 1566 abstracts, seven of which were included in the systematic review. The interventions for reducing ADEs included prescription or medication reviews by a pharmacist (n = 4), primary care physician (n = 1) or research team (n = 1), and an educational intervention (n = 1) for nursing staff to improve the recognition of potentially harmful medications and corresponding ADEs. Meta-analysis found no statistically significant benefit from any interventions on hospitalisation, ED visits, mortality, QoL or mental health and physical function.
Conclusions
No significant benefit was gained from any of the interventions in terms of the outcomes considered. New approaches are required to reduce ADEs in older adults.



Similar content being viewed by others

Change history
27 January 2020
Unfortunately, the co-author name was incorrectly published as ‘ ‘Lamona’’ instead of ‘ ‘Lamorna’’ in the original article
References
Nebeker J, Barach P, Samore M. Clarifying adverse drug events: a clinician’s guide to terminology, documentation, and reporting. Ann Intern Med. 2004;140(10):795–801.
Gandhi T, Weingart S, Borus J, et al. Adverse drug events in ambulatory care. N Eng J Med. 2003;348:1556–64. https://doi.org/10.1056/nejmsa020703.
Beijer J, de Blaey C. Hospitalisations caused by adverse drug reactions (ADR): a meta-analysis of observational studies. Pharm World Sci. 2002;23(2):46–54 (PMID:12061133).
Pirmohamed M, James S, Meakin S, et al. Adverse drug reactions as cause of admission to hospital: prospective analysis of 18,820 patients. BMJ. 2004;329:15.
Oscanoa TJ, Lizaraso F, Carvajal A. Hospital admissions due to adverse drug reactions in the elderly. A meta-analysis. Eur J Clin Pharmacol. 2017;73(6):759–70. https://doi.org/10.1007/s00228-017-2225-3.
Hohl C, Dankoff J, Colacone A, Afilalo M. Polypharmacy, adverse drug-related events, and potential adverse drug interactions in elderly patients presenting to an emergency department. Ann Emerg Med. 2001;38(6):666–71.
Laroche M, Charmes J, Nouaille Y, Picard N, Merle L. Is inappropriate medication use a major cause of adverse drug reactions in the elderly? Br J Clin Pharmacol. 2007;63:177–86.
Onder G, Petrovic M, Tangiisuran B, et al. Development and validation of a score to assess risk of adverse drug reactions among in-hospital patients 65 years or older: the GerontoNet ADR risk score. Arch Intern Med. 2010;170:1142–8.
Batel Marques F, Penedones A, Mendes D, Alves C. A systematic review of observational studies evaluating costs of adverse drug reactions. Clinicoecon Outcomes Res. 2016;8:413–26. https://doi.org/10.2147/ceor.s115689.
Spinewine A, Fialova D, Byrne S. The role of the pharmacist in optimizing pharmacotherapy in older people. Drugs Ageing. 2012;29:495–510.
Hohl C, Bohdan N, Kuramoto L, et al. Outcomes of emergency department patients presenting with adverse drug events. Ann Emerg Med. 2011;58(270–279):e4. https://doi.org/10.1016/j.annemergmed.2011.01.003.
Higgins JPT, Sterne JAC, Savović J et al. A revised tool for assessing risk of bias in randomized trials In: Chandler J, McKenzie J, Boutron I, Welch V (editors). Cochrane Methods. Cochrane Database of Systematic Reviews 2016; Issue 10 (Suppl 1). dx.doi.org/https://doi.org/10.1002/14651858.cd201601.
Gallagher P, Ryan C, Byrne S, Kennedy J, O’Mahony D. STOPP (Screening Tool of Older Person’s Prescriptions) and START (Screening Tool to Alert doctors to Right Treatment). Consensus validation. Int J Clin Pharmacol Ther. 2008;46:72–83.
American Geriatrics Society 2012 Beers Criteria Update Expert Panel (2012). American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2012;60(4):616–31.
Hanlon JT, Schmader KE, Samsa GP, Weinberger M, Uttech KM, Lewis IK, et al. A method for assessing drug therapy appropriateness. J Clin Epidemiol. 1992;45:1045–51.
Pitkala K, Juola A, Kautiainen H, et al. Education to reduce potentially harmful medication use among residents of assisted living facilities: a randomized controlled trial. JAMDA. 2014;15:892–8.
Frankenthal D, Lerman Y, Kalendaryev E, Lerman Y. Intervention with the Screening tool of older persons potentially inappropriate prescriptions/Screening Tool to Alert Doctors to right Treatment Criteria in elderly residents of a chronic geriatric facility: a randomized clinical trial. JAGS. 2014;62:1658–65.
Campins L, Serra-Prat M, Gozalo I, on behalf of the REMEI Group, et al. Randomized controlled trial of an intervention to improve drug appropriateness in community-dwelling polymedicated elderly people. Fam Pract. 2017;34:36–42. https://doi.org/10.1093/fampra/cmw073.
Touchette D, Masica A, Dolor R, et al. Safety-focussed medication therapy management: a randomized controlled trial. J Am Pharm Assoc. 2012;52:603–12.
Hanlon J, Weinberger M, Samsa G, et al. A randomized, controlled trial of a clinical pharmacist intervention to improve inappropriate prescribing in elderly outpatients with polypharmacy. Am J Med. 1996;100:428–37.
Yeh Y, Liu C, Peng L, Lin M, Chen L. Potential benefits of reducing medication-related anticholinergic burden for demented older adults: a prospective cohort study. Geriatr Gerontol Int. 2013;13:694–700.
Olsson I, Runnamo R, Engfeldt P. Drug treatment in the elderly: an intervention in primary care to enhance prescription quality and quality of life. Scan J Prim Health C. 2012;30:3–9.
Garratt A, Schmidt L, Mackintosh A, Fitzpatrick R. Quality of life measurement: bibliographic study of patient assessed health outcome measures. BMJ. 2002;324:1417–21.
Formica D, Sultana J, Cutroneo P, et al. The economic burden of preventable adverse drug reactions: a systematic review of observational studies. Expert Opin Drug Saf. 2018;17(7):681–95.
Kucukarslan S, Peters M, Mlynarek M, Naafziger D. Pharmacists on rounding teams reduce preventable adverse drug events in hospital general medicine units. Arch Intern Med. 2003;163:2014–8.
Riordan DO, Walsh KA, Galvin R, Sinnott C, Kearney PM, Byrne S. The effect of pharmacist-led interventions in optimising prescribing in older adults in primary care: a systematic review. SAGE Open Med. 2016. https://doi.org/10.1177/2050312116652568.
Avery A, Rodgers S, Cantrill J, et al. A pharmacist-led information technology intervention for medication errors (PINCER): a multicentre, cluster randomised, controlled trial and cost-effectiveness analysis. Lancet. 2012;379(9823):1210–9.
Clyne B, Smith SM, Hughes CM, Boland F, Cooper JA, Fahey T. Sustained effectiveness of a multifaceted intervention to reduce potentially inappropriate prescribing in older patients in primary care (OPTISCRIPT study). Implement Sci. 2016;11:79. https://doi.org/10.1186/s13012-016-0442-2.
Cooper JA, Cadogan CA, Patterson SM, et al. Interventions to improve the appropriate use of polypharmacy in older people: a Cochrane systematic review. BMJ Open. 2015;5:e009235. https://doi.org/10.1136/bmjopen-2015-009235.
Khalil H, Bell B, Chambers H, Sheikh A, Avery A. Professional, structural and organisational interventions in primary care for reducing medication errors. Cochrane Database Syst Rev. 2017. https://doi.org/10.1002/14651858.cd003942.pub3.
Acknowledgements
The authors acknowledge Paul Murphy, medical library in RCSI, who assisted with the searches in the systematic review.
Author information
Authors and Affiliations
Contributions
KB, CC and CB prepared the protocol on the review; CB, CC, ST refined the search terms; CB, ST and LB reviewed abstracts and full papers with CC; ST, KB and CC conducted analysis. All involved in the interpretation and preparation of the manuscript.
Corresponding author
Ethics declarations
Funding
KB, CC, CB and ST were funded by a Health Research Board (HRB) Research Leader Award (HRB-RL-2015-1579). The sponsor had no role in the design, methods, data collection, analysis and preparation of the paper.
Conflict of interest
Sarah Tecklenborg, Catherine Byrne, Caitriona Cahir, Lamorna Brown and Kathleen Bennett have no conflicts of interest that are directly relevant to the content of this article.
Data Availability
The datasets generated and analysed during the current study are available from the corresponding author on reasonable request.
Additional information
The original version of this article was revised: The co-author name was corrected to “Lamorna” in the original article.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Tecklenborg, S., Byrne, C., Cahir, C. et al. Interventions to Reduce Adverse Drug Event-Related Outcomes in Older Adults: A Systematic Review and Meta-analysis. Drugs Aging 37, 91–98 (2020). https://doi.org/10.1007/s40266-019-00738-w
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40266-019-00738-w