
ABSTRACT
BACKGROUND
Racial and ethnic disparities in opioid prescribing in the emergency department (ED) are well described, yet the influence of socioeconomic status (SES) remains unclear.
OBJECTIVES
(1) To examine the effect of neighborhood SES on the prescribing of opioids for moderate to severe pain; and (2) to determine if racial disparities in opioid prescribing persist after accounting for SES.
DESIGN
We used cross-sectional data from the National Hospital Ambulatory Medical Care Survey between 2006 and 2009 to examine the prescribing of opioids to patients presenting with moderate to severe pain (184 million visits). We used logistic regression to examine the association between the prescribing of opioids, SES, and race. Models were adjusted for age, sex, pain-level, injury-status, frequency of emergency visits, hospital type, and region.
MAIN MEASURES
Our primary outcome measure was whether an opioid was prescribed during a visit for moderate to severe pain. SES was determined based on income, percent poverty, and educational level within a patient’s zip code.
RESULTS
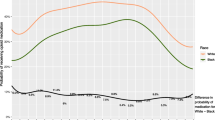
Opioids were prescribed more frequently at visits from patients of the highest SES quartile compared to patients in the lowest quartile, including percent poverty (49.0 % vs. 39.4 %, P < 0.001), household income (47.3 % vs. 40.7 %, P < 0.001), and educational level (46.3 % vs. 42.5 %, P = 0.01). Black patients were prescribed opioids less frequently than white patients across all measures of SES. In adjusted models, black patients (AOR 0.73; 95 % CI 0.66–0.81) and patients from poorer areas (AOR 0.76; 95 % CI 0.68–0.86) were less likely to receive opioids after accounting for pain-level, age, injury-status, and other covariates.
CONCLUSIONS
Patients presenting to emergency departments from lower SES regions were less likely to receive opioids for equivalent levels of pain than those from more affluent areas. Black and Hispanic patients were also less likely to receive opioids for equivalent levels of pain than whites, independent of SES.

Similar content being viewed by others

Abbreviations
- NAMCS:
-
National Ambulatory Medical Care Survey
- NHAMCS:
-
National Hospital Ambulatory Medical Care Survey
- NCHS:
-
National Center for Health Statistics
- CDC:
-
Center for Disease Control and Prevention
- NDC:
-
National Drug Code
- ED:
-
Emergency Department
REFERENCES
Manchikanti L, Singh A. Therapeutic opioids: a ten-year perspective on the complexities and complications of the escalating use, abuse, and nonmedical use of opioids. Pain Physician. 2008;11:S63–88.
Fortuna R, Robbins BW, Caiola E, Joynt MR, Halterman JS. Prescribing of controlled medications to adolescents and young adults in the United States. Pediatrics. 2010;126(6):1108–16.
Phillips DM. JCAHO pain management standards are unveiled. Joint Commission on Accreditation of Healthcare Organizations. JAMA. 2000;284:428–9.
Pletcher MJ, Kertesz SG, Kohn MA, Gonzales R. Trends in opioid prescribing by race/ethnicity for patients seeking care in US emergency departments. JAMA. 2008;299(1):70–8.
Todd KH, Samaroo N, Hoffman JR. Ethnicity as a risk factor for inadequate emergency department analgesia. JAMA. 1993;269(12):1537–9.
Epstein AM, Ayanian J. Racial disparities in medical care. NEJM. 2001;344(19):1471–3.
Bazarian JJ, Pope C, McClung J, Cheng YT, Flescher W. Ethnic and racial disparities in emergency department care for mild traumatic brain injury. J Acad Emerg Med. 2003;10(11):1209–17.
National Center for Health Statistics. NCHS public-use data files and documentation: National Hospital Ambulatory Medical Care Survey (NHAMCS)—2006, 2007, 2008, 2009. Available at: ftp://ftp.cdc.gov/pub/health_statistics/nchs/dataset_documentation/nhamcs.
Pollack CE, Mallya G, Polsky D. The impact of consumer-directed health plans and patient socioeconomic status on physician recommendations for colorectal cancer screening. J Gen Intern Med. 2008;23(10):1595–601.
Green CR, Ndao-Brumblay SK, West B, Washington T. Differences in prescription opioid analgesic availability: comparing minority and white pharmacies across Michigan. J Pain. 2005;6(10):689–99.
Bradley CJ, Given CW, Roberts C. Race, socioeconomic status, and breast cancer treatment and survival. JNCI J Natl Cancer Inst. 2002;94(7):490–6.
Madison T, Schottenfeld D, James SA, Schwartz AG, Gruber SB. Endometrial cancer: socioeconomic status and racial/ethnic differences in stage at diagnosis, treatment, and survival. Am J Public Health. 2004;94:2104–11.
Cooper R, Cutler J, Desvigne-Nickens P, Fortmann SP, Friedman L, Havlik F, Hogelin G, Marler J, McGovern P, Morosco G, Mosca L, Pearson T, Stamler J, Stryer D, Thom T. Trends and disparities in coronary heart disease, stroke, and other cardiovascular diseases in the United States: findings of the national conference on cardiovascular disease prevention. Circulation. 2000;102:3137–47.
Meara ER, Richards S, Cutler DM. The gap gets bigger: changes in mortality and life expectancy, by education, 1981–2000. Heal Aff. 2008;27(2):350–60.
Le H, Ziogas A, Lipkin SM, Zell JA. Effects of socioeconomic status and treatment disparities in colorectal cancer survival. Cancer Epidemiol Biomarkers Prev. 2008;17(8):1950–62.
Tamayo-Sarver JH, Dawson NV, Hinze SW, Cydulka RK, Wigton RS, Albert JM, Ibrahim SA, Baker DW. The effect of race/ethnicity and desirable social characteristics on physicians’ decisions to prescribe opioid analgesics. Acad Emerg Med. 2003;10(11):1239–48.
Komaromy M, Grumbach K, Drake M, Vranizan K, Lurie N, Keane D, Bindman AB. The role of black and Hispanic physicians in providing health care for underserved populations. N Engl J Med. 1996;334(20):1305–10.
Rabinowitz HK, Diamond JJ, Veloski JJ, Gayle JA. The impact of multiple predictors on generalist physicians’ care of underserved populations. Am J Public Health. 2000;90(8):1225–8.
Cooper LA, Powe NR. Disparities in patient experiences, health care processes, and outcomes: the role of patient-provder racial, ethnic, and language concordance. The Commonwealth Fund, July 2004.
Berger JT. The influence of physicians’ demographic characteristics and their patients’ demographic characteristics on physician practice: implications for education and research. J Assoc Am Med Coll. 2008;83(1):100–5.
Sequist TD, Fitzmaurice GM, Marshall R, Marston A, Safran DG, Ayanian JZ. Cultural competency training and performance reports to improve diabetes care for black patients: a cluster randomized, controlled trial. Ann Intern Med. 2010;152:40–6.
Glymour MM, Saha S, Bigby JA. Physician race and ethnicity, professional satisfaction, and work-related stress: results from the Physician Worklife Study. Natl Med Assoc. 2004;96(10):1283–9. 1294.
U. S. Census Bureau. Per capita statistics: United States. Retrieved April 11, 2012. From http://www.census.gov/statab/ranks/rank29.html;2000.
Heins A, Grammas M, Heins JK, Costello MW, Huang K, Mishra S. Determinants of variation in analgesic and opioid prescribing practice in an emergency department. J Opioid Manag. 2006;2(6):335–40.
Dormuth CR, Miller TA, Huang A, Mamdani MM, Juurlink DN. Canadian drug safety and effectiveness research network. Effect of a centralized prescription network on inappropriate prescriptions for opioid analgesics and benzodiazepines. Can Med Assoc J. 2012;184(16):E852–6.
Reifler LM, Droz D, Bailey JE, et al. Do prescription monitoring programs impact state trends in opioid abuse/misuse? Pain Manag. 2012;13:434–42.
Financial Disclosures
None.
Conflict of Interest
The authors declare that they do not have any conflicts of interest.
Contributor’s Statement
All authors made substantial contributions to the conception and design, interpretation of data, drafting and revising of the manuscript, and final approval for publication.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Joynt, M., Train, M.K., Robbins, B.W. et al. The Impact of Neighborhood Socioeconomic Status and Race on the Prescribing of Opioids in Emergency Departments Throughout the United States. J GEN INTERN MED 28, 1604–1610 (2013). https://doi.org/10.1007/s11606-013-2516-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-013-2516-z