
Abstract
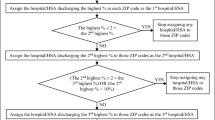
Hospitals need to understand patient flows in an increasingly competitive health economy. New initiatives like Patient Choice and the Darzi Review further increase this demand. Essential to understanding patient flows are demographic and geographic profiles of health care service providers, known as ‘catchment areas’ and ‘catchment populations’. This information helps Primary Care Trusts (PCTs) to review how their populations are accessing services, measure inequalities and commission services; likewise it assists Secondary Care Providers (SCPs) to measure and assess potential gains in market share, redesign services, evaluate admission thresholds and plan financial budgets. Unlike PCTs, SCPs do not operate within fixed geographic boundaries. Traditionally, SCPs have used administrative boundaries or arbitrary drive times to model catchment areas. Neither approach satisfactorily represents current patient flows. Furthermore, these techniques are time-consuming and can be challenging for healthcare managers to exploit. This paper presents three different approaches to define catchment areas, each more detailed than the previous method. The first approach ‘First Past the Post’ defines catchment areas by allocating a dominant SCP to each Census Output Area (OA). The SCP with the highest proportion of activity within each OA is considered the dominant SCP. The second approach ‘Proportional Flow’ allocates activity proportionally to each OA. This approach allows for cross-boundary flows to be captured in a catchment area. The third and final approach uses a gravity model to define a catchment area, which incorporates drive or travel time into the analysis. Comparing approaches helps healthcare providers to understand whether using more traditional and simplistic approaches to define catchment areas and populations achieves the same or similar results as complex mathematical modelling. This paper has demonstrated, using a case study of Manchester, that when estimating the catchment area of a planned new hospital, the extra level of detail provided by the gravity model may prove necessary. However, in virtually all other applications, the Proportional Flow method produced the optimal model for catchment populations in Manchester, based on several criteria: it produced the smallest RMS error; it addressed cross-boundary flows; the data used to create the catchment was readily available to SCPs; and it was simpler to reproduce than the gravity model method. Further work is needed to address how the Proportional Flow method can be used to reflect service redesign and handle OAs with zero or low activity. A next step should be the rolling out of the method across England and looking at further drill downs of data such as catchment by Healthcare Resource Group (HRG) rather than specialty level.





Similar content being viewed by others
References
Bailey NTJ (1956) Statistics in hospital planning and design. Appl Stat 5(2):146–157
Bailey TC, Gatrell AC (1995) Interactive spatial data analysis. Longman Scientific & Technical
Bikker JA, de Vos AF (1992) A regional supply and demand model for inpatient hospital care. Environ Plann A 24(8):1097–116
Congdon P (2001) The development of gravity models for hospital patient flows under system change: a bayesian modelling approach. Health Care Manage Sci 4(4):289–304
Congdon P, Best N (2000) Small area variation in hospital admission rates: Bayesian adjustment for primary care and hospital factor. Appl Stat 49(2):207–226
Cooper Z, Gibbons S, Jones S, McGuire A (2010) Does hospital competition improve efficiency? Paper No’ CEPDP0988, An Analysis of the Recent Market-Based Reforms to the English NHS, LSE Centre for Economic Performance, Download from http://cep.lse.ac.uk/_new/publications/abstract.asp?index=3620.
Flowers J (2003) Catchment areas and populations [online]. INphoRM, February 2003 Issue 2. Available at: http://www.erpho.org.uk/download.aspx?urlid=9480&urlt=1 (Accessed 07/03/11).
Flowers J (2005) Catchment areas and populations - a lost art. June 10. [lecture] Eastern Regional Public Health Observatories. Available online at: http://www.erpho.org.uk/download.aspx?urlid=12449&urlt=1 (Accessed 07/03/11).
Gandy RJ (1979) The calculation of catchment population within the National Health Service. Statistician 28(1):29–36
Gu W, Wang X, McGregor SE (2010) Optimization of preventive health care facility locations. International Journal of Health Geographics 9(17). Available online at: http://www.ij-healthgeographics.com/content/9/1/17 (accessed 09/01/11).
Harper PR (2002) A framework for operational modelling of hospital resources. Health Care Manage Sci 5(3):165–173
Harper PR, Shahani AK (2003) A decision support system for the care of HIV and AIDS patients in India. Eur J Oper Res 147(1):187–197
Harper PR (2005) Planning health services with explicit geographical considerations: a stochastic location-allocation approach. Omega 33(2):142–152
Harper PR, Phillips S, Gallagher JE (2005) Geographical simulation modeling for the regional planning of oral and maxillofacial surgery across London. J Oper Res Soc 56(2):134–143
Health and Social Care (Community Health and Standards) Act (2003) Available online at: http://www.opsi.gov.uk/acts/acts2003/ukpga_20030043_en_1 (accessed 14/07/10).
Huff DL (1964) Defining and Estimating a Trading Area. J Mark 28(3):34–38
Lippi Bruni M, Nobilio L, Ugolini C (2008) The analysis of a cardiological network in a regulated setting: a spatial interaction approach. Health Econ 17(2):221–33
Lowe JM, Sen A (1996) Gravity model applications in health planning: analysis of an urban hospital market. J Reg Sci 36(3):437–461
Mayer JD (1983) The distance behavior of hospital patients: a disaggregated analysis. Soc Sci Med 17(12):819–827
Mayhew LD, Gibberd RW, Hall H (1986) Predicting patient flows and hospital case-mix. Environ Plann A 18(5):619–638
Morrill RL, Earickson RJ (1968) Hospital Variation and Patient Travel Distances. Inquiry V(4):26–34, published by the Blue Cross Blue Shield Association, Chicago, Illinois
Morrill RL, Earickson RJ, Rees P (1970) Factors Influencing distances traveled to hospitals. Econ Geogr 46(2):161–171
Morrill RL, Kelley MB (1970) The simulation of hospital use and the estimation of location efficiency. Geogr Anal 2:283–300
Norris V (1952) Role of statistics in regional hospital planning with special reference to the Birmingham hospital region. Br Med J 1(4750):129–133
Office for National Statistics (2007) Beginner’s guide to UK geography: census geography. Available online at: http://www.statistics.gov.uk/geography/census_geog.asp (accessed 10/01/11)
Oliveira MD (2004) Modelling demand and supply influences on utilization: a flow demand model to predict hospital utilization at the small area level. Appl Econ 36(20):2237–2251
Oliveira MD, Bevan G (2006) Modelling the redistribution of hospital supply to achieve equity taking account of patient’s behaviour. Health Care Manage Sci 9(1):19–30
Reilly WJ (1931) The law of retail gravitation. Knickerbocker, New York
Senn SJ (1981) Some comments on “The calculation of catchment populations within the National Health Service”. Statistician 30(1):73–75
Senn SJ, Samson WB (1982) Estimating hospital catchment populations. Statistician 31(1):81–96
Shewan J (2003) Catchment areas and populations. INphoRM, (2, February 2003) [online]. Available at: http://www.erpho.org.uk/download.aspx?urlid=9480&urlt=1 (accessed 14/07/10)
Skidmore S (1981) Some Comments on the “Calculation of catchment populations within the National Health Service” by Gandy. Statistician 30(1):69–72
Taket AR (1989) Equity and Access: exploring the effects of hospital location on the population served—a case study in strategic planning. J Oper Res Soc 40(11):1001–1009
Wilson RM, Gibberd RW (1990) Allocating resources between health care regions: catchment populations and allocating for equity. Eur J Oper Res 49(3):333–347
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jones, S., Wardlaw, J., Crouch, S. et al. Modelling catchment areas for secondary care providers: a case study. Health Care Manag Sci 14, 253–261 (2011). https://doi.org/10.1007/s10729-011-9154-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10729-011-9154-y