
Abstract
Background Compared with the general population, autistic adults experience higher rates of physical and mental health conditions, premature morbidity and mortality, and barriers to health care. A health check for autistic people may improve their health outcomes.
Aim To establish the views of autistic people towards a primary care health check for autistic people.
Design & setting Cross-sectional questionnaire study in England and Wales.
Method A questionnaire was sent to autistic adults with physical health conditions in England and Wales. A total of 458 people (441 autistic adults and 17 proxy responders) completed the questionnaire.
Results Most responders (73.4%, n = 336) thought a health check is needed for all autistic people. Around half of the participants thought a health check should be offered from childhood and the health check appointment should last between 15 and 30 minutes. Autistic people were positive about providing primary care staff with contextual information regarding their health and the reasonable adjustments they would like before their health check appointment. Training about autism and the health check was considered important, alongside adequate time for discussions in the health check appointment (all by over 70% of responders). The clinician’s autism knowledge, seeing a familiar clinician, environmental adaptations, appropriate information, and accessible appointments were considered particularly important in making a health check accessible.
Conclusion Autistic people and relatives were supportive of a primary care health check for autistic people. Information gathered was used to support the design of a primary care health check for autistic adults.
How this fits in
Compared with the general population, autistic adults experience higher rates of health conditions, premature morbidity and mortality, and barriers to effective health care. Strong support was found for a primary care health check for autistic adults, and important information was given about health check design and delivery. Most responders thought the health check should be available to all autistic adults. Autistic people thought consideration of personalised reasonable adjustments would improve acceptability and access to the health check.
Introduction
Autism research has started to systematically investigate co-occurring mental and physical health conditions, and healthcare access for autistic people.1,2 Large scale studies have found an increased prevalence of health conditions in autistic people versus population samples, independent of whether intellectual disability is present.3–7 For example, autistic adults seem more likely to experience premature mortality from neoplasms, endocrine conditions, and conditions of the nervous, circulatory, and respiratory systems.8,9
Studies highlight barriers faced by autistic adults accessing health care including the following: waiting areas that cause sensory overload;10,11 problems with patient–provider communication;12 a lack of training about autism among healthcare providers;13 and cognitive difficulties.14,15 For example, difficulties with executive functioning impacting on follow-up of care, missing appointments owing to memory difficulties, and translating medical care into concrete actions.15–17 These factors may increase distress throughout the healthcare experience (for example, when travelling to healthcare appointments, waiting for and during the appointment) that only reduces after returning home.11 Barriers likely contribute to difficulties identifying and treating autistic adults’ health conditions. In the UK, adjustments to healthcare service provision may be available; however, a recent study showed a gap between adjustments autistic people want from services and what was received.18
Annual health checks specifically designed for people with intellectual disability have been developed and evaluated in randomised controlled trials.19,20 In England, a health check for people with intellectual disabilities has been integrated into primary care. A review of health checks for people with intellectual disabilities found they consistently detected unmet health needs and led to targeted actions to address needs.21 Autistic people with co-occurring intellectual disabilities may receive a health check for people with intellectual disabilities; however, this health check is not available to (and may not be appropriate for) the significant proportion of autistic people who do not have co-occurring intellectual disabilities. Recent healthcare policy in England has advocated for the development and evaluation of health checks specifically designed to meet the needs of all autistic people (NHS Long Term Plan and National Strategy for Autistic Children, Young People and Adults).22,23 A health check for all autistic adults that incorporates adjustments to health care may help to overcome barriers to access, reduce health inequalities, improve health, and reduce early mortality for autistic people with and without intellectual disability.
This health checks research programme was conceived at a workshop to establish priority research areas to improve the physical health and wellbeing of autistic people.24 The research aimed to investigate the views of autistic people about a specifically designed health check, the important features of design and delivery, and what would make accessing a health check easier (or more challenging). The study methods and materials were co-designed with autistic people and relatives as part of a wider programme of co-produced research (https://research.ncl.ac.uk/autismhealthchecks).
Method
Participants
Recruitment was through the Adult Autism Spectrum Cohort-UK (ASC-UK),25 an ongoing, longitudinal study of the lived experiences of UK autistic adults; any UK-based autistic person aged ≥16 years is able to participate in ASC-UK. Cohort recruitment was through any source, including health providers, voluntary sector, and community organisations. All ASC-UK participants aged ≥18 years who provided baseline data identifying they had one or more physical health condition (for example, diabetes, hypertension, asthma, arthritis), and lived in England or Wales were eligible to be contacted. All autistic adults with capacity to do so had given consent to be re-contacted; autistic adults who could not give informed consent for themselves were represented by a relative or carer authorised to act on their behalf (termed a ‘proxy responder’).25,26
Materials
The research team (which includes autistic people) designed the survey, and autistic people who were not part of the study team were consulted about content and piloted the survey. Responders' demographic information was available from ASC-UK (data access supported by ASC-UK chief investigator Dr Jeremy Parr). The survey included the following: items about a health check for autistic adults, including provision (Do you think regular health checks for autistic people should be provided?); and delivery (At what age do you think health checks should be offered? How often should they be carried out? How long would you expect a health check for autistic people to last? How would you like to be told what to expect from a health check specifically for autistic adults? Would you be happy to provide information about your health needs before the health check? Would you be happy to provide information about any reasonable adjustments you’d like before the health check?). Questions also focused on health check delivery and implementation (What would make health checks easier for autistic adults or harder for autistic adults?).
Most questions offered fixed-choice responses; there were opportunities for free-text responses (for example, to elaborate on reasons for response selection or add information). Participants were asked to provide up to three free-text responses regarding what would make health check access easier and three free-text responses regarding what would make a health check harder).
Procedure
Eligible participants were sent an information sheet and survey by post or email. The electronic version of the survey was hosted on Qualtrics.27 Participants could contact the research team for assistance completing the questionnaire (one participant made use of this). A reminder was sent to eligible participants after 1 month.
Analysis
Data from autistic people and proxy responders were grouped together for analysis.
To investigate representativeness, responders and non-responders were compared (using χ2 tests) on age (18–25 years, 26–40 years, 41–60 years, ≥61 years), sex (male and female), and preferred contact method (post or email).
Summary statistics were calculated for closed survey questions. Several questions allowed for multiple options to be selected, meaning that the number of responses could be greater than the number of participants. To explore systematic differences in responses, comparisons were made by the following: sex (male and female, 14 participants did not report a sex of male or female and were excluded from sex comparisons only); by age; and by intellectual disability. Post-hoc comparisons were not carried out because there were insufficient participants within groups.
Content analysis was completed for free-text responses; an inductive approach was used.28 HT read responses and created categories to organise data. HT and DM separately coded data, assigning responses to categories. Any differences in categorisation were discussed, and agreement reached. Where responses did not fit into a category, further categories were created. HT and DM further reviewed the categories and condensed these into 17 final categories. Each response from each participant was coded separately. The number of responses within each category were expressed as a proportion of the total responses (excluding non-codable responses). Non-codable responses included: expressions of uncertainty; ambiguous responses not attributable to a category, such as 'pre-conceptions' or 'lack of knowledge'; answers unrelated to the topic; or answers stating no opinion.
Results
A total of 1001 people (944 autistic adults and 57 proxy responders) were contacted and 458 people consented to take part (46%, n = 441 autistic adults, and n = 17 proxy responders). Participant characteristics are described in Table 1.
Responders and non-responders
Responders and non-responders were rather similar; nevertheless, owing to group size, there were some statistically significant differences between the groups (see Table 2).
Quantitative responses
Responses relating to the importance and content of the health check are summarised in Table 3.
It was found that 73.4% of participants (n = 336) thought that a regular health check should be provided, with only 5.0% (n = 23) not wanting a regular health check, and 12.0% (n = 55) being unsure. There were no differences in these proportions for sex (all χ2 P values ≥0.05), but there was a significant effect of age and intellectual disability. As part of a health check, the majority of participants (86.9%, n = 398) were willing to provide information about their health needs. Similarly, 86.2% of responders (n = 395) said they would provide information on the reasonable adjustments they would like. There were no age, sex, or intellectual disability effects associated with responses to these items (see Tables 3 4).
Responses showed a clear preference for primary care staff to be trained in autism, and delivering a health check for autistic people (rated ‘very important’ by n = 365 responders (79.7%) and n = 324 responders (70.7%) respectively). Autistic people thought that a health check should be available online and on paper, with only a minority thinking this was not important (n = 72, 15.7% for online; n = 59, 12.9% for paper). Finally, over-three quarters (77.1%, n = 353) thought having adequate time for discussions was ‘very important’ (Table 3). Although there were no age or intellectual disability effects associated with these responses, there was a sex effect when participants were asked about the need for all staff involved in the health check to receive training about autism.
Most people (67.9%, n = 311) wanted a health check to be for all autistic people, irrespective of whether they had intellectual disabilities. Only nine responders (2.0%) reported that it should only be for people without intellectual disability. There were no differences in these proportions for sex (all χ2 P-values ≥0.05), or intellectual disability, but there was a significant effect of age.
67.3% of responders (n = 308) thought a health check should be available from childhood or the teenage years; 5% (n = 24) thought health checks should start from age ≥40 years.
There was a strong preference for an annual health check (61.4%, n = 281). Half of the responders (50.7%, n = 232) thought a health check should last for 15–30 minutes (options ranged from <15 minutes to >45 minutes). Just over half of responders wanted to be contacted about a health check by letter (54.6%, n = 250). There were no age, sex, or intellectual disability effects associated with these responses.
Open-text responses and categories
Inter-rater reliability
Cohen’s Kappa was used to estimate inter-rater reliability. For both open-text questions, percentage agreement and Kappa statistic were high. For the facilitators question data, Cohen’s Kappa was 0.965 (96.9% agreement, P<0.001). For the barriers question data, Cohen’s Kappa was 0.904 (91.7% agreement, P<0.001).
What would make a health check easier to access?
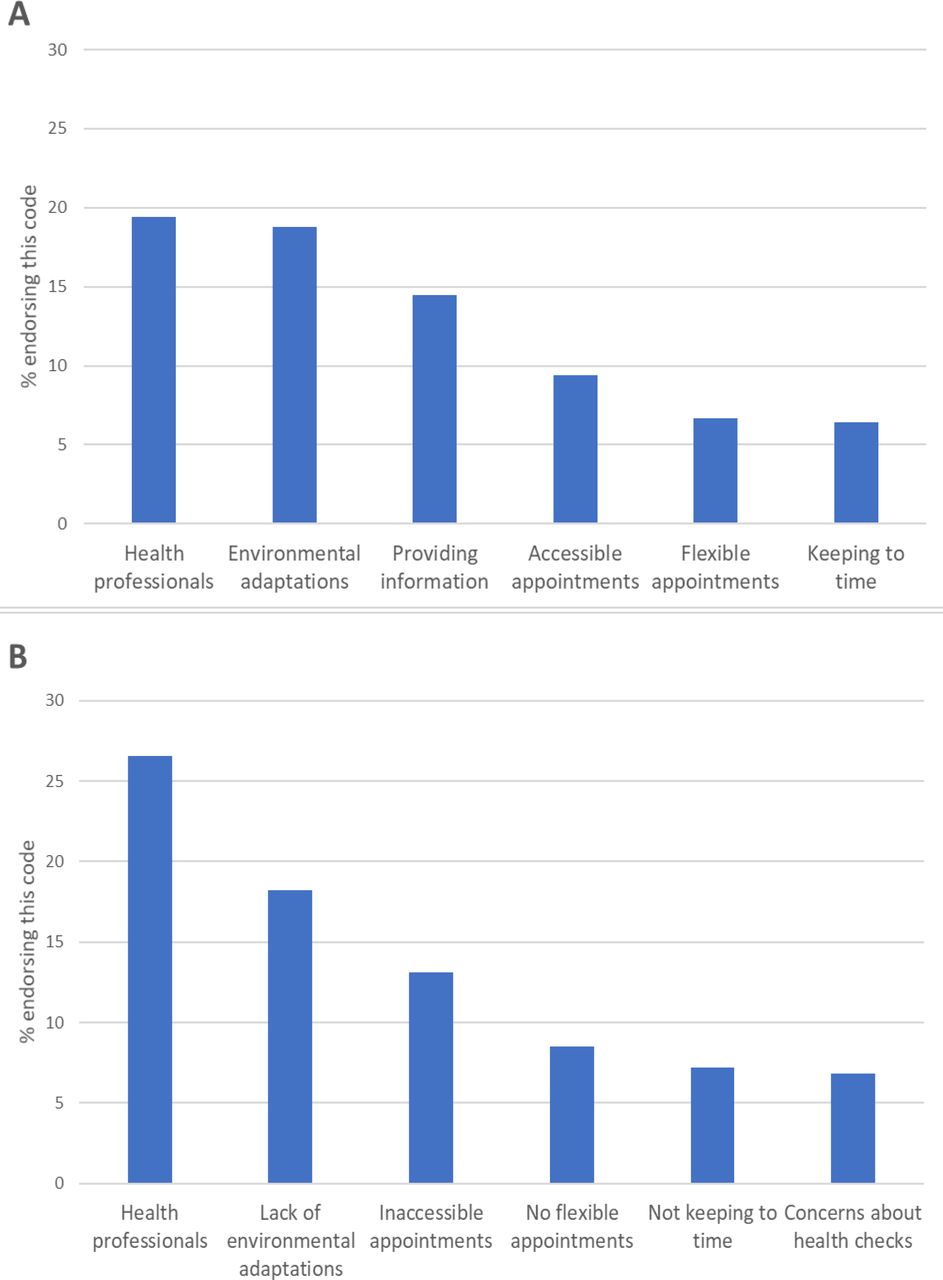
Supplementary Table S1 lists the response categories and illustrative anonymised quotations for each of the categories. The most frequent responses about what would make a health check easier were: factors relating to health professionals, such as a familiar clinician, and/or someone who knows about autism (19.5%, n = 171); environmental factors such as low-level sensory stimulation, especially in the waiting room (18.9%, n = 166); and providing information about the health check, such as who the participant will be seen by, photographs of the venue and staff, and information about what will happen (14.6%, n = 128) (see Figure 1). Responders also identified specific requirements of the health check (5.0%, n = 44), including offering adjustments, doing health checks online, health professionals reviewing notes beforehand, and having a written summary detailing the outcomes of the appointment.
{kind=link}
What would make a health check more challenging to access?
The responses were consistent with those reported above, with health professionals (26.5%, n = 215) and environmental factors (18.1%, n = 147) listed as the biggest potential challenges to a health check (see Figure 1). Responses indicated that health professionals could make health checks more challenging for reasons by being 'patronising' or 'not knowledgeable about autism'. Other factors included inaccessible appointments (for example, inflexibility with appointment times and locations; 13.1%, n = 106) and factors related to the organisation of the appointment, such as a lack of support or unclear communication. Only 6.8% (n = 55) reported concerns about the health check appointment itself (for example, being put on the spot to answer questions, being pressured to attend, long forms to complete on the day and undertaking physical assessments without seeking consent, such as measuring blood pressure).
Discussion
Summary
The study represents a first step in the authors' research programme to co-design and evaluate a health check for autistic adults, and to address this aim of the UK NHS Long Term Plan.23 The findings suggest strong support from autistic people for a health check and provide useful information for its design and delivery in primary care. The majority thought a health check should be available for all autistic people, irrespective of intellectual ability, and include consideration of personalised reasonable adjustments to improve access to health care, with flexible delivery methods to maximise acceptability.
Open-text responses identified some key factors relevant to a health check for autistic people, and these could apply more generally to healthcare encounters. Specifically, flexible ways of booking appointments (for example, booking online avoiding a phone call) and providing advance information about the health check were perceived as facilitators for access. Incorporating these factors into the development of a health check for autistic adults may increase uptake.
Strengths and limitations
The large survey included autistic people from a wide age range including 61 people aged ≥61 years (13.3%), a group whose views are often missing from the autism literature.29,30 Through ASC-UK recruitment, it was possible to include a large number of female participants in this study. The age and sex distribution allowed the authors to investigate sex and age effects, although both factors could not be considered simultaneously. Demographic information, including sex, was gathered from ASC-UK and the response options were based on advice received from autistic people. As such, the authors are not able to comment on whether the findings are generalisable to people who do not report as male or female; this group may face additional challenges accessing health care and more research is needed to investigate what maximises good healthcare access. Finally, proxy responders were included in the analyses, but the views of those with intellectual disability were under-represented; further exploration is needed to help inform health check implementation. The open-text responses were necessarily brief; interviews and focus groups focusing on this topic are also part of the health check development process and are reported elsewhere.31
Comparison with existing literature
The findings are in agreement with previous literature that finds some factors impact negatively on healthcare access.11,12,15 Autistic adults emphasised the importance of health professionals having a good understanding of autism, as is also identified elsewhere.12 A lack of professionals’ understanding may lead to autistic people being less satisfied with patient–provider communication,32 which could be to the extent that health conditions are not identified.30 A final consideration is continuity of GP or practice nurse seen. This is important in health care generally,33 but may be particularly relevant for autistic people.34
Implications for research and practice
Considering the aims of the NHS Long Term Plan and autistic adults’ views here, evaluating a health check specifically designed for autistic adults is an appropriate next step. A subsequent trial of its clinical and cost effectiveness is planned, and if demonstrated, the study results will be important for those considering implementation in primary care. Future studies to investigate health check use for autistic people in other countries will be important, as provision will need to be made appropriate for other health systems.
Notes
Funding
This study was funded by the Inge Wakehurst Trust who funded the Improving the Health of Older Autistic People study, and the UK autism research charity Autistica and the Peter Sowerby Foundation (reference:7257) who funded the Health Checks for Autistic Adults study.
Ethical approval
A favourable opinion for this study was given by Wales Research Ethics Committee 5 Bangor (18/WA/0191). Survey completion was taken as informed consent.
Provenance
Freely submitted; externally peer reviewed.
Acknowledgements
The authors are grateful to all the participants who gave their time to take part in the study. The authors are also grateful to Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust for acting as research sponsor, external advisory group members, and steering committee members for the autism spectrum adulthood and ageing programme.
Competing interests
The authors declare that no competing interests exist.
- Received May 5, 2022.
- Revision received May 5, 2022.
- Accepted May 6, 2022.
- Copyright © 2022, The Authors
This article is Open Access: CC BY license (https://creativecommons.org/licenses/by/4.0/)
References
In this issue








Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...
