
Abstract
Background A more comprehensive understanding and measurement of adult social care need could contribute to efforts to develop more effective, holistic personalised care, particularly for those with multiple long-term conditions (MLTC). Progress in this area faces the challenge of a lack of clarity in the literature relating to how social care need is assessed and coded within variables included in primary care databases.
Aim To explore how social care need is assessed and coded within variables included in primary care databases.
Design & setting An exploratory rapid scoping review of peer-reviewed articles and grey literature.
Method Articles were screened and extracted onto a charting sheet and findings were summarised descriptively. Articles were included if published in English and related to primary and social care using data from national primary care databases.
Results The search yielded 4010 articles. Twenty-seven were included. Six articles used the term ‘social care need’, although related terminology was identified including ‘need factors’, ‘social support’, and ‘social care support’. Articles mainly focused on specific components of social care need, including levels of social care usage or service utilisation and costs incurred to social care, primary care, and other providers in addressing needs. A limited range of database variables were found measuring social care need.
Conclusion Further research is needed on how social care need has been defined in a UK context and captured in primary care big databases. There is potential scope to broaden the definition of social care need, which captures social service needs and wider social needs.
How this fits in
Relatively few studies have examined social care need, despite the availability of longitudinal records collating millions of variables on both health and social care. Understanding which variables are available to capture social care need, how these are recorded in practice, and standardising of coding could be useful in progressing research in this area. A more comprehensive understanding and measurement of adult social care need could potentially contribute to efforts to develop more effective, holistic personalised care, particularly for those with MLTC, who often have complex needs requiring a range of joined-up health and social care services, as well as wider social interventions.
Introduction
The burden of managing long-term conditions remains an overarching challenge for healthcare systems in the UK and worldwide.1,2 An unprecedented rise in life expectancy coupled with changes in lifestyle has resulted in an increase in the prevalence of chronic conditions such as cardiovascular diseases, hypertension, depression, and rheumatoid arthritis.2 This has seen the number of individuals developing ≥2 long-term chronic conditions rise substantially. MLTC is commonly associated with ageing, with more than two-thirds of adults aged ≥65 years having ≥2 long-term chronic conditions.3,4 A rising MLTC burden is also evident among those aged ≤45 years who reside in socioeconomically deprived areas.1 People with MLTC face numerous challenges, such as functional decline, higher disability, poorer mental health, as well as an overall reduced quality of life.5 Studies show that people with MLTC have the highest level of health service use and healthcare expenditure. For example, care and support provided for MLTC account for >50% of all primary and secondary care costs,6 primarily as a result of high levels of health service utilisation, in particular GP appointments, emergency service use, admissions, and medication use.2,7,8 In response, this has necessitated service integration to more holistically address the needs of people with multiple conditions.8 Compared with individuals with a single condition, those with MLTC often require a combination of both health and social care services.9
Both conceptually and in practice, it can be difficult to clearly distinguish between healthcare need and social care need. This review used the national framework for NHS continuing health care and NHS-funded nursing care10 to define and differentiate social care need and healthcare need. Healthcare need is defined in the framework as ‘the treatment, control, management or prevention of a disease, illness, injury or disability, and the care or aftercare of a person with these needs (whether or not the tasks involved have to be carried out by a health professional)’. Although there is not a formal legal definition of social care need in the UK, it can be described as ‘one that is focused on providing assistance with activities of daily living, maintaining independence, social interaction, enabling the individual to play a fuller part in society, protecting them in vulnerable situations, helping them to manage complex relationships and (in some circumstances) accessing a care home or other supported accommodation’.11 Importantly, this definition of social care need encompasses both a person’s social care provision needs and their wider social needs, which enable full participation in society.
Compared with healthcare need in people with MLTC,3,7,8 research evidence on social care need is more limited, largely as a result of a lack of clarity both in the literature and in practice of how to define and measure social care need. Despite the availability of longitudinal records collating millions of variables on both health and social care, there is uncertainty in the literature on standardisation of variables to capture ‘social care need’ and its related coding systems. Understanding which variables are available to capture social care need, how these are recorded in practice, and standardising of coding could be useful in progressing research in this area. Accordingly, an exploratory rapid scoping review was conducted to identify and gain a broad overview of the key research evidence relating to how social care need is assessed and coded within variables included in primary care databases.
Method
Review approach
The study followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines for scoping reviews.12 The scoping review method was used as it allowed for a rapid mapping of key existing evidence and sources available in an emerging field of research.13 Analytically, the scoping review primarily focused on the variables that are used to capture social care need, how these are recorded in practice, and standardised in coding.
Search strategy
Systematic electronic searches were conducted from inception to 26 October 2021 on the following electronic databases: MEDLINE, Embase, the Cochrane Library, Web of Science, the Cumulative Index to Nursing and Allied Health Literature (CINAHL), Trip Database, Social Care Online, and Social Sciences Citation Index. For searches of electronic databases, free-text and MeSH terms were used and limited to ‘primary care’ and ‘social care’. Details of search terms are available in Table 1. Manual searching of bibliographies were also conducted. The views of topic experts were also sought to identify additional sources.
Inclusion and exclusion criteria
Articles were eligible for inclusion if published in the English language, were geographically located in the UK, and were focused on primary and social care. Quality assessment criteria are not a priority for scoping reviews,13 therefore extracted articles were not excluded on this basis.
Study selection and data extraction
All articles identified were imported into the Rayyan collaborative review platform for screening, which was conducted in blinding mode. Rayyan enabled rapid screening of retrieved sources. Titles and abstracts were screened, with each article assessed for relevance according to the inclusion criteria. Full-text articles were retrieved. Both screening and data extraction were conducted independently by two reviewers and disagreement resolved by discussion. A data-charting form was used to collate the studies and identify key characteristics (see Supplementary Appendix S1). Reviewers extracted the article reference and date, the stated aim of the study, results, and variables or indicators that had been used to capture ‘social care need’. Any disagreement between reviewers about study or variable inclusion was resolved through discussion until a consensus was reached.
Summarising and analysis
The data gathered by the review were iteratively synthesised descriptively, through the use of counts to summarise article characteristics (that set out the number, type, and quality of studies extracted and collated social care need variables identified), the data-charting technique, and interpretation of the findings by sifting and sorting material.14 The main social care need variables identified were collated and are presented in Supplementary Appendix S1.
Results
Screening, inclusion, and exclusion of studies
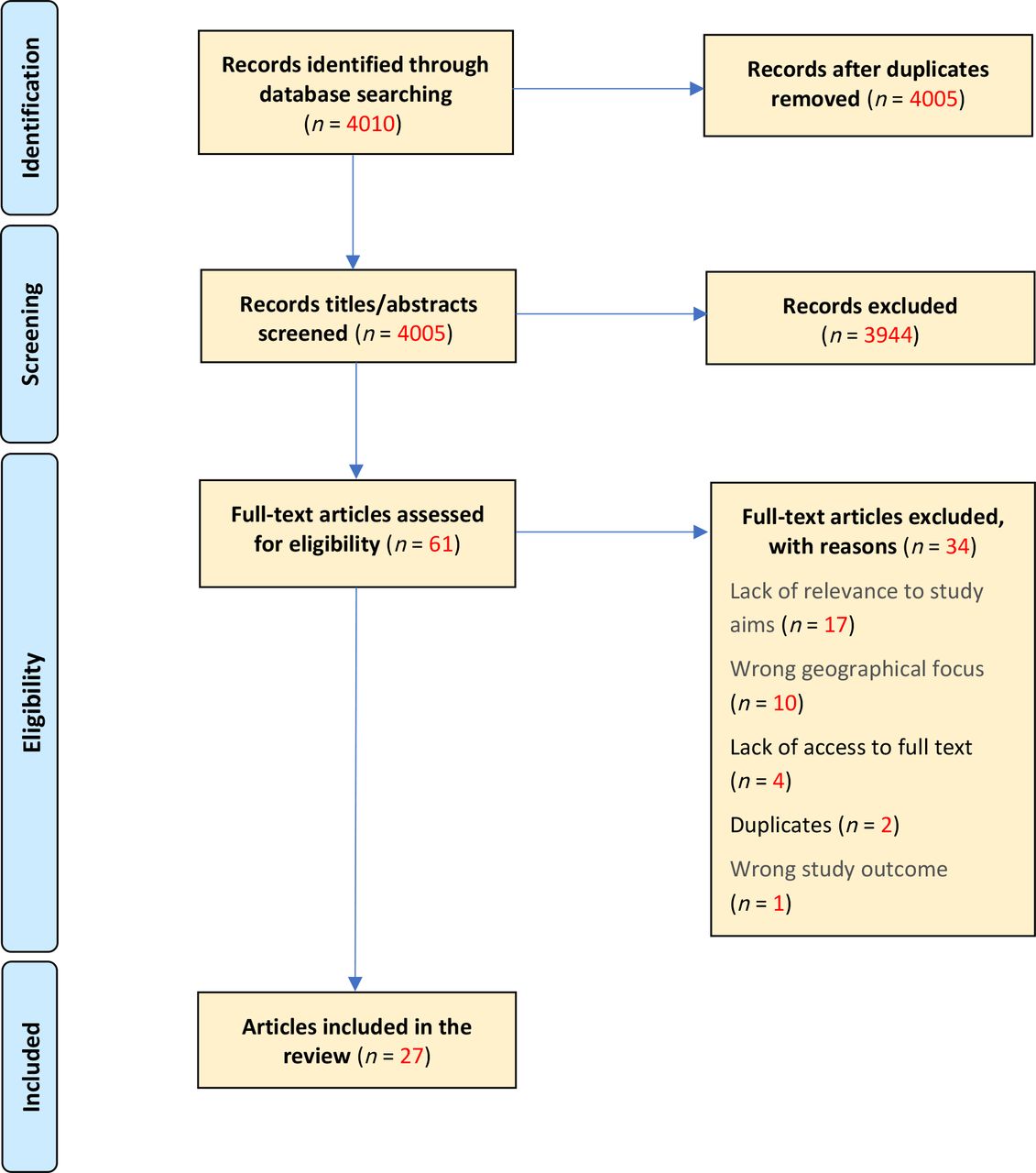
A total of 4010 articles were found by the review. After title and abstract screening using the Rayyan review tool, 61 articles were eligible for full-text screening. Following full-text screening, a further 34 articles were excluded, for reasons including:
did not produce findings or discuss the scoping review’s aim of how social care need is assessed and coded within variables included in primary care databases;
the geographical focus was not on the UK; and
the reviewers were unable to retrieve the full-text version of a small number of articles in the time available for the scoping review owing to publisher access permissions or paywalls.
A total of 27 final articles were included in the review.15–41 The flowchart of the screening process used for the review, including reasons for exclusion, are summarised in Figure 1.

{kind=link}
Characteristics of included studies
Most studies were located in the UK (n = 24),15–32,34–39 with a small number of UK and international studies identified (n = 3).33,40,41 Included articles were published between 2000 and 2021. The main study settings identified were either primary and/or secondary care, social care, or both. The main population groups examined in the studies were people with health conditions (patients) (n = 9),21,24,29,33,34,37–41,41 people in age categories ≥55 years (n = 5),18,19,28,37,40 service users (n = 3),23,27,32 and staff or healthcare professionals (n = 3).22,27,33 The most frequent sources of data used by studies were secondary data (n = 16),15–35,37–39,41,31,35,37–39,41 which is pooled data from primary sources, and primary data (n = 9).22–26,27,29,32,33,36,36
The main study designs used were cross-sectional (n = 5),16,30,33,38,40 mixed methods (n = 5),22,23,27,32,33 cohort study (n = 4),15,18,24,36 longitudinal (n = 3),22,29,33 systematic reviews (n = 2),21,35 and policy or evidence reviews (n = 2).25,41 A small number of studies were specifically based on datasets extracted from UK primary care databases including Clinical Practice Research Datalink (n = 2)16,35 and Secure Anonymised Information Linkage Databank (n = 2).17,18
Social care need(s)
Six studies specifically referred to the term ‘social care need’ although no standardised definition of social care need was identified.19,21,25–33,33 There were three studies using terms related to social care need, including ‘need factors’ (n = 1),28 ‘social support’ (n = 1),29 and ‘social care support’ (n = 1).23 Fifteen studies examined specific aspects of social care need, measuring the level of social care use or service utilisation (n = 8)15,19,22,23,28,33,34,36 and the costs of and the expenditure incurred to social care, primary care, and other care sectors or providers in addressing social care need (n = 7).24,27,29–32,39
The review found a relatively limited sample of studies containing data variables or coding lists from UK primary care database studies.15–18 These are shown in Supplementary Appendix S1. One study19 set out indicators measuring five aspects of ‘social care need’: ‘visual or hearing impairment, social isolation, access to an unpaid carer, activities of daily living/functional markers, other health problems recorded in social care data’. Another investigated the ‘recording of social factors in linked electronic health records of individuals aged ≥65 years, to assess the potential of these data to identify the social determinants of disease burden and uptake of healthcare interventions’.16 This study used a number of indicators to measure ‘social factors’, including ‘religion, ethnicity, immigration status, small area-level deprivation, place of residence (including communal establishments such as care homes), marital status and living arrangements (e.g. living alone, cohabitation)’.16 Reeve and Baker,20 albeit in the context of population health need, used a number of social care need-related indicators (described as ‘indices of social care provision’), which were focused on older people: ‘gross SSA [Social Security Administration] expenditure on elderly people per capita 75 years and over; people supported in residential/nursing care; the number of home help/care contact hours; and households receiving intense home care’.
The social care-related quality of life (SCRQoL) framework was used by some studies,21,22 which is based on the eight outcome domains of social care-related quality of life set out in the Adult Social Care Outcomes Toolkit. This was employed as an indicator of the quality of life of social care service users and to measure the outcomes and benefits of service provision, and specific interventions.23,24
Other indicators or measures utilised as surrogates of social care need included: ‘activities of daily living’ or ‘functional markers’ of need (for example, personal care, walking, bathing, or dressing);19 indicators measuring service utilisation (for example, home care, day care, and meals usage based on the number of days per year); using adult social care assessment to identify and measure demand for services; and, access to or presence of an unpaid or informal carer.19,25,26 One study27 that evaluated reablement outcomes used a questionnaire to ask service users if they felt they had ‘enough money to live on’, which acted as a ‘proxy indicator’ of their perceived financial situation in the context of understanding the impacts of wider social determinants of health.
Discussion
Summary
This rapid scoping review was conducted to identify and gain a broad overview13 of the key research evidence relating to how social care need is assessed and coded within variables included in primary care big databases. The study also sought to identify the range and type of ‘social care need’ variables or indicators used in the existing research literature. A common definition of social care need was not evident across included studies. Indeed, there was limited evidence of the use of the specific term ‘social care need’ across the literature. Other related terminology was used to describe aspects of social care need in specific population cohorts and in the context of service provision such as ‘need factors’,28 ‘social support’,29 and ‘social care support’.23 This review identified studies with a narrow analytical focus on particular variables or aspects of care need. For example, some studies considered and framed care need in terms of the costs incurred to social care, primary care, and other care providers, and/or in relation to levels of social care usage or utilisation.15,19,20,28,30,31 A few studies20,25,27,32 specifically focused on need identified through statutory social care service provision or interventions (for example, reablement or home help). While others21,24,33 examined what could be described as wider socioeconomic need or social determinants affecting health and wellbeing (for example, employment status, deprivation or social gradient, personal or household financial situation, and barriers to accessing services).
Strengths and limitations
This is the first review, to the authors’ knowledge, that collates evidence on how social care need has been examined in UK primary care big database studies. This review permitted rapid collation of evidence across a number of databases, with the inclusion of manual searches and expert input. Search terms were purposely broad, aimed at a comprehensive search and overview of research in this field.
However, the broad search criteria may have omitted studies in more specific subject fields or subdisciplines. As the review aims were only focused on UK databases, it was appropriate that searches were limited to UK studies and those published in the English language, although this will have resulted in the omission of relevant international evidence. Robust double peer-review and data extraction were carried out, but as this is a scoping review a formal quality appraisal process of included works was not conducted. It is important to acknowledge that unlike systematic reviews, the scoping review method does not attempt to achieve comprehensive coverage of the available research evidence, rather ‘to map the concepts underpinning a research area and the main sources and types of evidence available’.13 Therefore, more research is needed to identify additional sources and relevant evidence to validate the findings of this scoping review and further understand this research topic more generally.
Comparison with existing literature
This scoping review highlighted the limited literature focused specifically on social care need and associated indicators or variables, particularly in relation to those found in primary care big databases. This limited evidence base makes it difficult to systematically compare the findings of this scoping review with the findings of previous studies.
The review indicates a lack of universal agreement in the literature on which definition to use when describing social care needs for adults, a finding replicated in other work.42 It confirms the findings of other research such as that suggesting activities of daily living (ADL) is frequently employed as a proxy indicator of social care need,43 and it is also a useful measure for distinguishing the degree and type of care needs.20 This measure, which is based on local authority assessment of social care need data, does not capture the full range of social care and wider social needs of individuals.42,43 As Dunatchik and colleagues43 remark, an ADL ‘based approach also has the limitation that it is very task-focused and may underplay the importance of other aspects of life such as social contact and maintaining a sense of purpose, which are outcomes under the Care Act 2014’. While the review found evidence of other measures associated with social care need, these were mainly ‘service indicators’ measuring the type of social care provision and levels of service utilisation, and ‘indicators of costs’ incurred to care providers,43 which are even narrower measures that fail to capture the full range of social care need identified in the Care Act 2014.
Implications for research and practice
The findings of this review highlight the need for further research on how social care need has been defined in a UK context and captured in primary care big databases. In relation to policy and practice, there is scope to broaden the definition of social care need, especially beyond ADL measures, and develop more comprehensive measures or indicators of social care need, capturing both the full range of social care service provision needs and wider social needs (including social determinants of health) experienced by individuals. A more comprehensive understanding and measurement of adult social care need could potentially contribute to efforts to develop more effective, holistic personalised care, particularly for those with MLTC, who have complex and diverse needs requiring a range of joined-up healthcare and social care services, as well as wider social interventions.
Notes
Funding
The Primary Care Research Centre at the University of Southampton is a member of the National Institute for Health and Care Research (NIHR) School for Primary Care Research and supported by NIHR funds. Hajira Dambha-Miller is an NIHR-funded Academic Clinical Lecturer and has received NIHR funding for this grant (reference: NIHR202637). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the UK NIHR or the Department of Health and Social Care. Andrew Farmer receives support from NIHR Oxford BioMedical Research Centre.
Ethical approval
Ethical approval was not required for this scoping review.
Availability of data and materials:
Data used during the current study are available from the corresponding author on reasonable request.
Author contributions
GS and HDM conceived the study, LK and GS carried out data extraction and wrote the first draft of the paper. All authors contributed towards data interpretation and critically editing the manuscript.
Data
Data used during the current study are available from the corresponding author on reasonable request.
Provenance
Freely submitted; externally peer reviewed.
Acknowledgements
Competing interests
Hajira Dambha-Miller is the Editor-in-Chief of BJGP Open, but had no involvement in the peer review process or decision on this manuscript. All other authors have declared no competing interests.
Disclosure
The authors report no conflicts of interest in this work
- Received February 9, 2022.
- Revision received April 29, 2022.
- Accepted June 28, 2022.
- Copyright © 2022, The Authors
This article is Open Access: CC BY license (https://creativecommons.org/licenses/by/4.0/)
References
In this issue








Jump to section
More in this TOC Section
Related Articles
Cited By...
