
Article Figures & Data
Figures
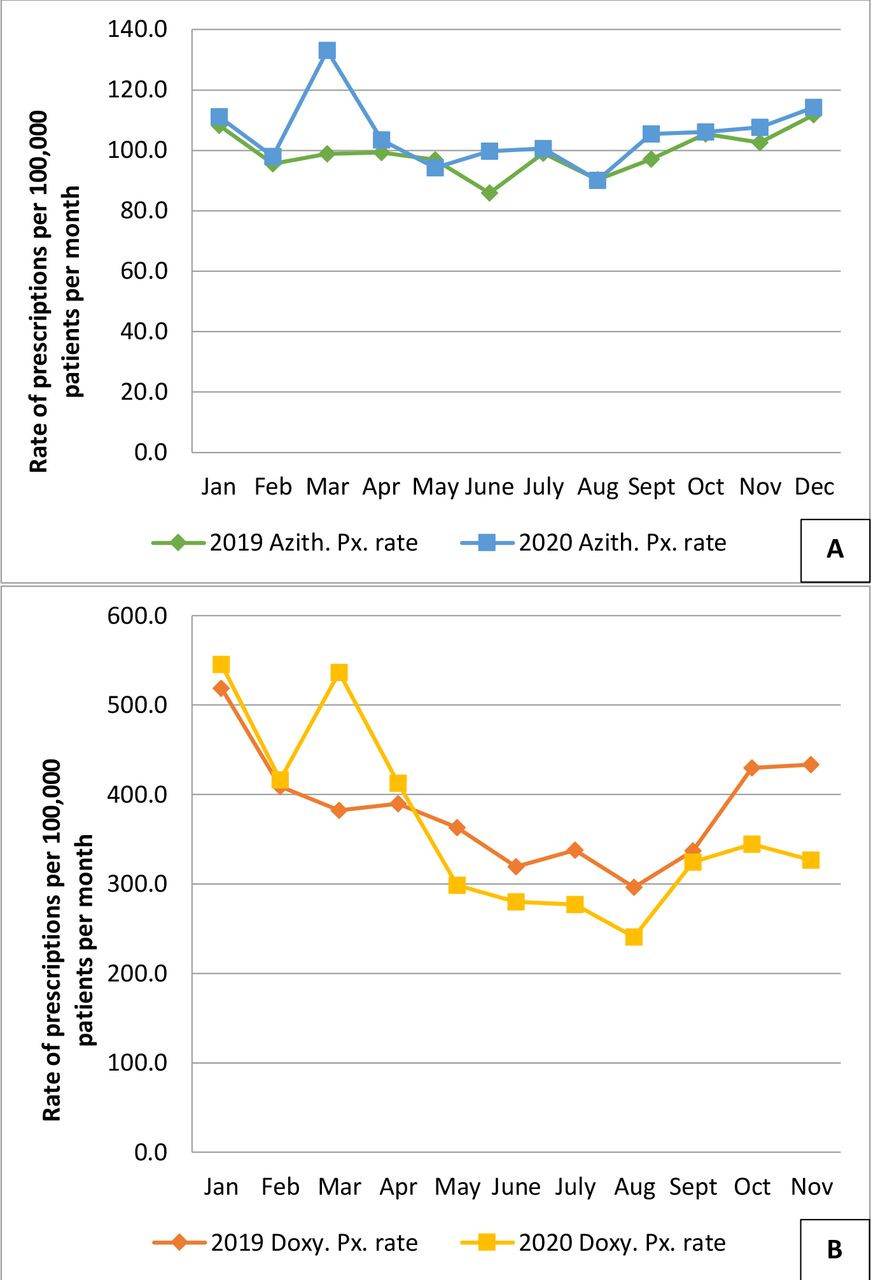
- Figure 1. Prescribing of azithromycin (Figure 1A) and doxycycline (Figure 1B) by month within the Research and Surveillance Centre. The 2020 prescription of both antibiotics (azithromycin = blue line, square markers; doxycycline = yellow line, square markers) was very similar in January and February to 2019 rates (azithromycin = green line, diamond markers; doxycycline = orange line; diamond markers). In March 2020, there was a peak of prescribing for both antibiotcs, coincident with the first wave of the COVID-19 pandemic. Thereafter azithromycin was prescribed in 2020 at or above the level in 2019, whereas doxycycline was prescribed less.
Azith = azithromycin. Doxy = doxycycline. Px = prescribing.
- Figure 2. Comparison of monthly incidence of consultations for lower respiratory tract infections (Figure 2A), upper respiratory tract infections (Figure 2B), and influenza-like illness (Figure 2C), comparing 2020 with 2019 in the Research and Surveillance Centre dataset. There was a lower incidence of LRTI and URI in 2020 compared with 2019, with a small peak when pupils returned to school in September 2020. ILI peaked with the first wave of the COVID-19 pandemic, and also with the return to school.
ILI = influenza-like illness. RTI = lower respiratory tract infections. URTI = upper respiratory tract infections.
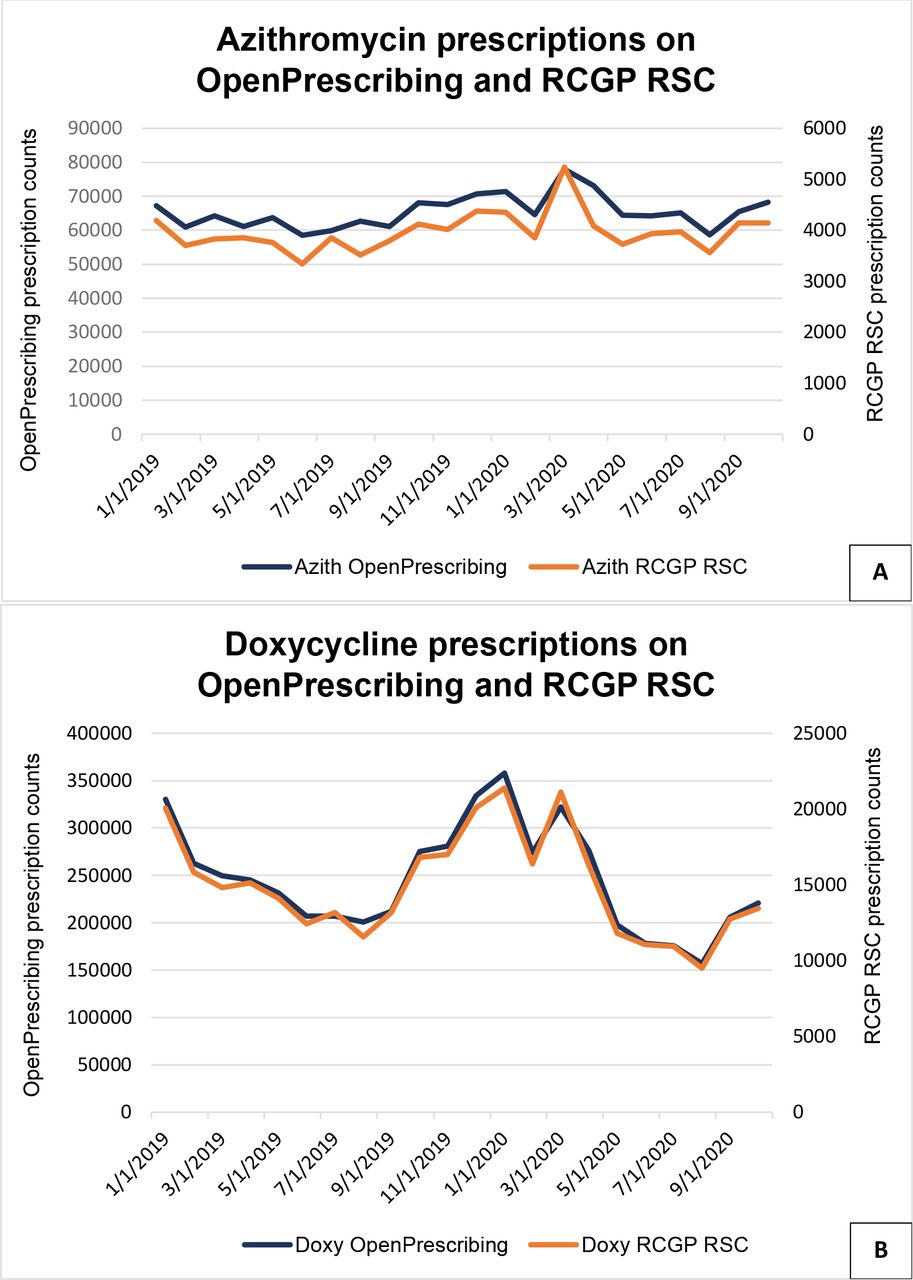
- Figure 3. Monthly pattern of azithromycin (Figure 3A) and doxycycline (Figure 3B) prescription counts, for 2019 and 2020. OpenPrescribing data are only available up to October 2020.
Azith = azithromycin. Doxy = doxycycline. RCGP RSC = Royal College of General Practitioners Research and Surveillance Centre.


{kind=link}
{kind=link}
{kind=link}
Tables
- Table 1. Comparison of rates of prescription of doxycycline and azithromycin in 2020 with 2019. In people aged ≥65 years there was a decrease in doxycycline use but an increase in azithromycin prescription. Lower respiratory tract infection and upper respiratory tract infection incidence fell across all age bands and both sexes. Influenza-like illness was much more similar between years.
Age, years 2019 2020 Female Male Female Male Antibiotic rates per 100000 patients (95% CI) Doxy. <16 21.74(20.4 to 23.2) 17.75(16.5 to 19.0) 19.12(17.8 to 20.5) 15.96(14.8 to 17.2) 16–64 385.28(382.1 to 388.5) 231.99(229.6 to 234.4) 380.15(377.8 to 383.3) 222.57(220.2 to 224.9) ≥65 1136.15(1126.4 to 1145.9) 1038.78(1028.6 to 1048.9) 968.28(959.3 to 977.3) 913.57(904.1 to 923.1) Azith. <16 56.89(54.6 to 59.2) 67.50(65.1 to 69.9) 53.29(51.1 to 55.5) 75.91(73.4 to 78.5) 16–64 70.02(68.7 to 71.4) 39.39(38.4 to 40.4) 70.69(69.4 to 72.1) 40.77(39.8 to 41.8) ≥65 305.17(300.1 to 310.3) 288.43(283.1 to 293.9) 339.13(333.8 to 344.5) 307.59(302.1 to 313.2) Respiratory disease rates per 100000 patients (95% CI) LRTI <16 229.25(224.67 to 233.82) 292.18(287.1 to 297.2) 68.43(65.9 to 70.9) 90.9(88.1 to 93.8) 16–64 191.30(189.1 to 193.54) 126.84(125.0 to 128.6) 81.45(79.9 to 82.9) 53.2(52.0 to 54.4) ≥65 609.27(602.05 to 616.5) 568.32(560.8 to 575.8) 267.9(263.2 to 272.8) 268.0(262.9 to 273.2) URTI <16 1320.33(1309.5 to 1331.3) 1349.86(1339.1 to 1360.7) 485.15(455.0 to 467.7) 493.1(486.6 to 499.7) 16–64 485.65(482.1 to 489.2) 229.3(226.9 to 231.8) 265.73(254.9 to 260.1) 117.38(115.7 to 119.1) ≥65 285.17(280.3 to 290.1) 208.6(204.1 to 213.2) 148.01(144.5 to 151.6) 104.61(101.4 to 107.9) ILI <16 19.30(17.1 to 19.7) 20.78(19.5 to 22.2) 16.38(15.2 to 17.7) 16.23(15.1 to 17.5) 16–64 32.57(30.8 to 32.6) 22.15(21.4 to 22.9) 37.68(36.7 to 38.7) 21.86(21.1 to 22.6) ≥65 25.40(28.2 to 31.7) 22.18(20.7 to 23.7) 29.41(27.9 to 31.0) 24.38(22.9 to 25.9) a95% confidence intervals. Azith = azithromycin. Doxy = doxycycline. ILI = influenza-like illness. LRTI = lower respiratory tract infections. URTI = upper respiratory tract infections.
- Table 2. Model reporting the incident rate ratio (IRR) comparing prescribing of azithromycin in 2020 with 2019. Taking the variables in the model into account there was a 22% increase, with people aged ≥65 years, female sex, the most deprived, northern regions and people with lower respiratory tract infections and upper respiratory tract infections all being associated with a higher rate of prescribing.
Azithromycin prescribing ratescomparing 2020 with 2019 IRR Lower Upper P 95% CI 95% CI Year 2020 (reference level: 2019) 1.22 1.19 1.26 <0.0001 Age band (reference level: 0–15) 16–64 0.71 0.68 0.73 <0.0001 ≥ 65 4.77 4.58 4.98 <0.0001 Sex (reference level: F) 0.91 0.88 0.93 <0.0001 IMD quintile (reference level: Q1, most deprived) Q2 0.90 0.86 0.94 <0.0001 Q3 0.87 0.83 0.90 <0.0001 Q4 0.75 0.72 0.78 <0.0001 Q5 (least deprived) 0.67 0.64 0.70 <0.0001 NHS region (reference: London) The Midlands and East 1.08 1.03 1.12 <0.0001 North East and Yorkshire 1.47 1.40 1.54 <0.0001 North West 1.13 1.08 1.18 <0.0001 South East 0.94 0.89 0.98 <0.0001 South West 0.72 0.69 0.76 <0.0001 Respiratory disease LRTI count 1.0051 1.0043 1.0058 <0.0001 URTI count 1.0030 1.0026 1.0035 <0.0001 ILI count 1.0017 0.9982 1.0053 0.3400 ILI = influenza-like illness. IMD = Index of Multiple Deprivation. LRTI = lower respiratory tract infections. URTI = upper respiratory tract infections.
- Table 3. Azithromycin prescribing in cases of COVID-19. For each unit rise in COVID-19 cases there has been a 3% rise in azithromycin prescriptions. Aged ≥65 years, female sex, being more deprived, northern regions, lower respiratory tract infections or influenza-like-illness infections are all associated with a higher rate of prescribing.
Azithromycin prescribing rate IRR Lower Upper P 95% CI 95% CI COVID-19 confirmed count 1.03 1.02 1.03 <0.0001 Age band (reference level: 0–15) 16–64 0.25 0.20 0.31 <0.0001 ≥65 10.95 8.67 13.83 <0.0001 Sex (reference level: F) 0.54 0.45 0.65 <0.0001 IMD quintile (reference level: Q1 most deprived) Q2 0.54 0.41 0.72 <0.0001 Q3 0.41 0.31 0.55 <0.0001 Q4 0.54 0.41 0.72 <0.0001 Q5 (least deprived) 0.66 0.50 0.88 0.0048 NHS region (reference: London) The Midlands and East 5.73 4.28 7.69 <0.0001 North East and Yorkshire 12.88 9.18 18.07 <0.0001 North West 10.31 7.34 14.49 <0.0001 South East 2.82 2.01 3.96 <0.0001 South West 1.41 1.01 1.98 0.0453 Respiratory disease LRTI count 1.94 1.92 1.97 <0.0001 URTI count 0.89 0.88 0.90 <0.0001 ILI count 1.60 1.54 1.68 <0.0001 ILI = influenza-like-illness. IMD = Index of Multiple Deprivation. LRTI = lower respiratory tract infections. URTI = upper respiratory tract infections.
Supplementary Data
- BJGPO.2021.0087_Supp.pdf -
Supplementary material is not copyedited or typeset, and is published as supplied by the author(s). The author(s) retain(s) responsibility for its accuracy.
In this issue








Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...
