
Article Figures & Data
Figures
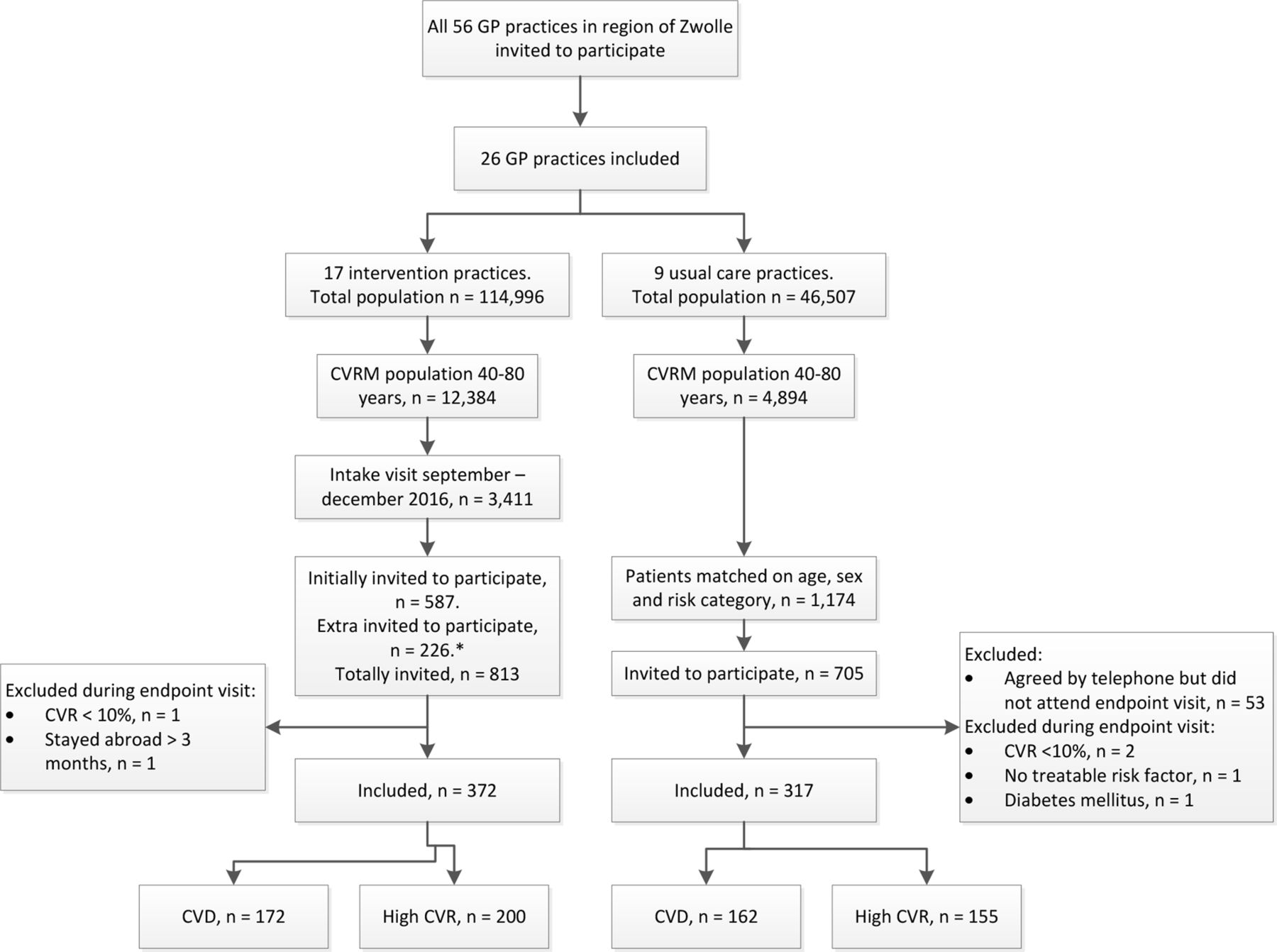
- Figure 1. ZWOT-CASE study flow diagram. CVD = cardiovascular disease. CVR = cardiovascular risk. CVRM = cardiovascular risk management. *As the response rate in the intervention group was lower than the expected 70%, the required sample size was not reached after 587 intervention patients were invited. Therefore, 226 extra patients were invited to the intervention group (total invited n = 813) and they were matched retrospectively to the usual care group.
{kind=link}
Tables
Characteristics Intervention group(n = 372) Usual care group(n = 317) Mean age, years (SD) 65.1 (8.3) 66.2 (7.5) Age <65 years 175 (47) 132 (42) Female 158 (42) 132 (42) Western 358 (96) 295 (93) Cardiovascular risk factors Hypertensiona 280 (75) 234 (74) Hypercholesterolemiaa 91 (24) 91 (29) Current smokerb 43 (12) 32 (10) Chronic kidney diseasec 40 (11) 51 (16) Microalbuminuriac 15 (4) 10 (3) Rheumatoid arthritisa 4 (1) 10 (3) Cardiovascular diseasesa,d 172 (46) 162 (51) Myocardial infarction 41 (11) 48 (15) Coronary sclerosis 46 (12) 44 (14) Angina pectoris 44 (12) 39 (12) Transient ischaemic attack 33 (9) 31 (10) Cerebral infarction 35 (9) 17 (5) Aneurysm aortae 8 (2) 11 (3) Intermittent claudication 12 (3) 13 (4) Atherosclerosis 4 (1) 4 (1) Comorbidities (including other CVD)a COPD 9 (2) 14 (4) Atrial fibrillation 23 (6) 16 (5) Heart failure 1 (0.3) 3 (1) Medication use b Antihypertensive agents 299 (80) 251 (79) Statins/lipid-lowering agents 190 (51) 167 (53) Anticoagulants 169 (45) 154 (49) Measurementse Mean SBP, mmHg (SD) 136.7 (15.2) — Mean DBP, mmHg (SD) 80.3 (9.5) — Mean LDL-cholesterol, mmol/l (SD) 2.8 (0.9) — Mean BMI (SD) 27.7 (4.0) — aBased on International Classification of Primary Care (ICPC)-coded diagnoses. bBased on medical records. cBased on ICPC-coded diagnoses and/or laboratory measurements. Microalbuminuria: albumin-creatinine ratio >3 mg/mmol. Chronic kidney disease: ≥3 months impaired renal function (estimated glomerular filtration rate <60 ml/minute/1.73 m2) and/or microalbuminuria.dCardiovascular diseases as inclusion criteria for integrated CVRM care and for the study. eBaseline measurements of the control group at t = 0 are not presented, as there was no routine intake consultation.
BMI = body mass index. COPD = chronic obstructive pulmonary disease. CVD = cardiovascular diseases. DBP = diastolic blood pressure. LDL = low-density lipoprotein. SBP = systolic blood pressure. SD = standard deviation.
Absolute numbers (%) are presented unless stated otherwise.
Outcomes Intervention group( n = 372) Usual care group( n = 317) Primary outcomes N N Mean systolic blood pressure, mmHg (SD) 358a 137.2 (16.2) 298b 139.0 (16.8) Mean LDL-cholesterol, mmol/l (SD) 347c 2.6 (0.8) 310d 2.6 (1.0) Secondary outcomes Mean diastolic blood pressure, mmHg (SD) 358 80.3 (10.2) 298 80.6 (10.1) Blood pressure <140/90 mmHg 358 214 (60) 298 175 (59) LDL-cholesterol <2.5 mmol/l 347 178 (51) 310 168 (54) LDL-cholesterol <1.8 mmol/le 166 45 (27) 163 58 (36) Smoking 363 31 (9) 311 30 (10) Mean BMI (SD) 349 27.3 (5.2) 300 27.7 (4.8) 10 -year CVD morbidity or mortality riskf All patients, median (IQR) 317 22.0 (11.7–36.4) 267 24.0 (13.7–38.0) Patients with CVD, median (IQR) 159 26.2 (17.9–38.5) 144 27.8 (18.7–39.5) Patients without CVD, median (IQR) 158 15.5 (5.4–31.9) 123 18.7 (8.4–34.3) Healthy food habits Vegetables >150–200 grams a day 360 142 (39) 294 99 (34) Fruits >200 grams a day 354 214 (60) 294 187 (64) Red meat <300 grams a week 356 207 (58) 286 155 (54) Fatty fish >1 a week 358 244 (68) 296 187 (63) Unhealthy fat products <3 a week & healthy fat products >3 a week 352 121 (34) 289 75 (26) Sweet & salty snacks <3 a week 357 196 (55) 295 157 (53) Table salt <3 a week 360 335 (93) 294 265 (90) Alcohol consumption, units a week, median (IQR) 311 3 (0–7) 292 2 (0–7) Physically activeg 303 230 (76) 250 178 (71) Medication use Patients with CVD Antihypertensive drugs 174 137 (79) 160 121 (76) Lipid-lowering drugs 174 139 (80) 160 127 (79) Anticoagulants 174 160 (92) 160 146 (91) Patients without CVD Antihypertensive drugs 187 167 (89) 149 126 (85) Lipid-lowering drugs 188 52 (28) 149 46 (31) GP as primary treating practitionerh 368 366 (99) 314 307 (98) Consultations in general practice, median (IQR)i 361 6 (3–10) 311 6 (3–10) Patient satisfaction (PREM) (1–5j), mean (SD) 359 3.6 (0.7) 283 3.5 (0.8) Recommendation score (0–10j), mean (SD) 352 8.3 (1.3) 275 8.2 (1.3) EQ-5D-5L index score (–0.45–1j), mean (SD) 353 0.9 (0.1) 290 0.8 (0.1) SF-12 Mental component (7.9–72.0j), mean (SD) 353 53.9 (7.5) 290 52.3 (9.3) SF-12 Physical component (5.2–64.7j), mean (SD) 353 48.1 (9.2) 290 46.7 (10.0) HADS Anxiety (0–7j), mean (SD) 342 4.1 (3.3) 286 4.5 (3.7) HADS Depression (0–7j), mean (SD) 347 3.2 (3.0) 283 3.9 (3.3) Newly developed CVDk 364 10 (3) 311 10 (3) Newly developed comorbidityl 363 13 (4) 311 12 (4) Mortality 372 5 (1) 318 3 (1) aReasons for missing data: died before endpoint (n = 5), not measured (n = 7), data not available owing to change of GP (n = 2). bReasons for missing data: died before endpoint (n = 3), not measured (n = 16). cReasons for missing data: died before endpoint (n = 5), not measured (n = 16), data not available owing to change of GP (n = 4). dReasons for missing data: died before endpoint (n = 3), not measured (n = 3), data not available owing to change of GP (n = 1). eFor patients with CVD, n = 175 in intervention group and n = 164 in usual care group. fFor patient with known CVD the SMART-function was used to calculate the risk; for patients without CVD the risk was based on the risk chart in the Dutch guideline for CVRM (based on the SCORE risk function).15 g >5 days a week moderate intense physical activity >30 minutes a day. hPrimary treating practitioner could be the GP or a medical specialist. iIncluding all visits and telephone calls with the general practice for all reasons. jMinimum and maximum possible values. kIncluding cardiovascular diseases as inclusion criteria for integrated CVRM care and for the study. lIncluding diabetes mellitus, chronic obstructive pulmonary disease, heart failure, atrial fibrillation, and chronic renal impairment.
BMI = body mass index. CVD = cardiovascular diseases. EQ-5D-5L = five-level EuroQoL-5 Dimensions. HADS = Hospital Anxiety and Depression Scale. IQR = interquartile range. LDL = low-density lipoprotein. PREM = Patient Reported Experience Measure. SD = standard deviation. SF-12 = Short Form–12 Health Survey.
Absolute numbers (%) are presented unless stated otherwise.
- Table 3. Effect of integrated CVRM care on the primary and secondary outcomes compared with usual care, using generalised mixed-model analyses
Crude modela Adjusted modelb Outcomes n Betac 95% CI P value n Betac 95% CI P value Primary outcomes Systolic blood pressure 656 –1.75 –5.78 to 2.29 0.38 647 –1.78 –6.09 to 2.53 0.40 LDL-cholesterol 657 0.05 –0.13 to 0.23 0.58 653 0.01 –0.15 to 0.18 0.86 Secondary outcomes, continuous Diastolic blood pressure 656 0.04 –3.05 to 3.13 0.97 647 –0.37 –3.78 to 3.04 0.82 BMI 649 –0.27 –1.28 to 0.74 0.59 641 0.09 –0.83 to 1.02 0.84 EQ-5D-5L index score 643 0.01 –0.02 to 0.04 0.46 633 0.01 –0.02 to 0.03 0.64 SF-12 Mental component 643 1.61 0.21 to 3.02 0.03d 633 1.39 –0.17 to 2.95 0.08 SF-12 Physical component 643 1.45 –0.38 to 3.28 0.12 633 1.01 –0.74 to 2.76 0.25 Patient satisfaction (PREM) 642 0.13 –0.03 to 0.29 0.11 631 0.14 –0.03 to 0.32 0.10 Recommendation score 627 0.13 –0.10 to 0.36 0.24 616 0.11 –0.13 to 0.36 0.35 HADS Anxiety 628 –0.39 –1.05 to 0.27 0.23 618 –0.35 –1.06 to 0.37 0.32 HADS Depression 630 –0.61 –1.27 to 0.06 0.07 620 –0.45 –1.19 to 4.41 0.22 n Ratio e 95% CI P value n Ratio e 95% CI P value Secondary outcomes, log transformed 10-year CV risk All patients 584 0.87 0.75 to 1.02 0.08 583 0.90 0.76 to 1.06 0.21 Patients with CVD 303 0.98 0.86 to 1.12 0.76 303 1.04 0.90 to 1.20 0.59 Patients without CVD 281 0.81 0.62 to 1.06 0.11 280 0.80 0.60 to 1.08 0.15 Secondary outcomes, dichotomous Blood pressure <140/90 mmHg 656 0.96 0.54 to 1.83 0.99 647 0.97 0.52 to 1.83 0.93 LDL-cholesterol <2.5 mmol/l 657 0.89 0.64 to 1.23 0.48 653 1.13 0.74 to 1.72 0.57 LDL-cholesterol <1.8 mmol/l 329 0.64 0.37 to 1.13 0.12 326 0.70 0.39 to 1.26 0.24 Smoking 674 0.87 0.52 to 1.48 0.62 671 1.00 0.54 to 1.85 0.99 Healthy food habitsf Vegetables 654 1.28 0.93 to 1.77 0.13 643 1.26 0.87 to 1.83 0.21 Fruits 648 0.88 0.64 to 1.20 0.41 637 0.94 0.65 to 1.35 0.72 Red meat 642 1.17 0.86 to 1.61 0.32 632 1.21 0.85 to 1.74 0.29 Fatty fish 654 1.30 0.89 to 1.91 0.18 643 1.24 0.83 to 1.85 0.30 Fatty products 641 1.49 1.06 to 2.11 0.02d 631 1.41 0.95 to 2.08 0.09 Snacks 652 1.07 0.79 to 1.46 0.67 641 1.22 0.85 to 1.73 0.28 Table salt 654 1.47 0.84 to 2.58 0.18 643 1.68 0.84 to 3.35 0.14 Physical activity 553 1.29 0.83 to 1.99 0.25 543 1.31 0.84 to 2.06 0.24 Medication use Patients with CVD Antihypertensive drugs 334 1.19 0.72 to 1.99 0.50 334 5.09 0.56 to 46.0 0.15 Lipid-lowering drugs 334 1.03 0.61 to 1.76 0.91 334 0.97 0.26 to 3.57 0.96 Anticoagulants 334 1.10 0.51 to 2.38 0.82 334 1.52 0.23 to 9.90 0.66 Patients without CVD Antihypertensive drugs 336 1.52 0.80 to 2.90 0.20 336 1.23 0.12 to 12.2 0.86 Lipid-lowering drugs 337 0.86 0.53 to 1.37 0.52 337 0.71 0.18 to 2.79 0.62 GP as primary treating practitioner 682 3.93 0.74 to 21.0 0.11 671 10.50 0.80 to 138.3 0.07 Newly developed CVD 675 0.85 0.35 to 2.07 0.72 671 0.99 0.37 to 2.64 0.99 Newly developed comorbidity 674 0.91 0.34 to 2.41 0.85 671 1.11 0.43 to 2.91 0.83 Mortality 689 1.48 0.32 to 6.89 0.62 672 0.37 0.00 to 38.8 0.68 Secondary outcomes, count Alcohol consumption 601 0.88 0.65 to 1.19 0.39 594 0.81 0.60 to 1.09 0.17 Consultations in general practice 672 1.05 0.89 to 1.25 0.54 670 1.04 0.89 to 1.21 0.65 aCorrected for clustering within practices. bCorrected for clustering within practices and predefined confounders. cDifference between intervention and usual care group. dStatistically significant. eRatio, should be interpreted as a multiplication factor. For example, a ratio of 1.05 should be interpreted as a 5% higher outcome score in the intervention group compared with the usual care group. fHealthy food habits: vegetables >150–200 grams a day; fruits >200 grams a day; red meat <300 grams a week; fatty fish >1 a week; unhealthy fatty products <3 a week and healthy fatty products >3 a week; sweet and salty snacks <3 a week; table salt <3 a week.
BMI = body mass index. CV = cardiovascular. CVD = cardiovascular disease. EQ-5D = five-level EuroQoL-5 Dimensions. HADS = Hospital Anxiety and Depression Scale. LDL = low-density lipoprotein. PREM = Patient Reported Experience Measure. SF-12 = Short Form–12 Health Survey.
In this issue








Jump to section
More in this TOC Section
Related Articles
Cited By...
