
Abstract
Background General practice in the UK faces continuing challenges to balance a workforce shortage against rising demand. The NHS England GP Forward View proposes development of the multidisciplinary, integrated primary care workforce to support frontline service delivery, including the employment of paramedics. However, very little is known about the safety, clinical effectiveness, or cost-effectiveness of paramedics working in general practice. Research is needed to understand the potential benefits and drawbacks of this model of workforce organisation.
Aim To understand how paramedics are deployed in general practice, and to investigate the theories and drivers that underpin this service development.
Design & setting A mixed-methods study using a literature review, national survey, and qualitative interviews.
Method A three-phase study was undertaken that consisted of: a literature review and survey; meetings with key informants (KIs); and direct enquiry with relevant staff stakeholders (SHs).
Results There is very little evidence on the safety and cost-effectiveness of paramedics working in general practice and significant variation in the ways that paramedics are deployed, particularly in terms of the patients seen and conditions treated. Nonetheless, there is a largely positive view of this development and a perceived reduction in GP workload. However, some concerns centre on the time needed from GPs to train and supervise paramedic staff.
Conclusion The contribution of paramedics in general practice has not been fully evaluated. There is a need for research that takes account of the substantial variation between service models to fully understand the benefits and consequences for patients, the workforce, and the NHS.
How this fits in
Despite the clear policy direction, very little is known about the safety, clinical effectiveness, and cost-effectiveness of paramedics working in general practice. Furthermore, there is limited information available about the different ways paramedics are deployed in general practice, and the intended benefits and unintended consequences of different workforce models. This scoping study explores the theories underpinning the deployment of paramedics in general practice services. The findings can be used to inform larger scale research on this subject.
Introduction
General practice services in the UK are facing an unprecedented recruitment and retention challenge. This is happening at a time when services are under increasing pressure owing to a growing and ageing population.1,2 The NHS England GP Forward View seeks to address workload issues in primary care by promoting a multidisciplinary approach. It proposes funding for 20 000 more staff to be enlisted to support GPs. These staff, including paramedics, are intended to free up GPs to spend more time with patients and enable practices to offer more services.3 Some of the perceived benefits of deploying paramedics in general practice are highlighted as the management of minor illnesses, undertaking home visits, and the provision of same-day ‘urgent’ primary care.4,5
Precise figures on the number of paramedics working in general practice are difficult to ascertain owing to the wide variety of employment models. However, the General Practice Workforce dataset indicates that numbers almost doubled between 2017 and 2018.6 Despite this, and the clear policy directive, very little is known about the safety, clinical-, or cost-effectiveness of paramedics working in general practice. Much of the existing literature focuses on which additional skills may be needed by paramedics to work autonomously and safely in general practice and other community settings.7–9 However, this research is largely descriptive and there are several assumptions, such as paramedics reducing GP workload and costs, which have not been tested empirically.
A particular challenge for general practice is embedding paramedics in the most appropriate way. Local need will, to some extent, dictate the types of patients seen, the clinical problems managed, and the relationships with other acute and community services.10 Different practice sizes, workforce composition, and demographics mean it is likely that a range of models are already in place. For example, paramedics may be employed directly by a practice or shared across a primary care network or clinical commissioning group (CCG). Some paramedics may be employed for specific tasks, while others may work more broadly in general practice. Before research can begin to determine the most appropriate ways of utilising paramedics in the general practice workforce, it is important to understand the extent of variation and associated drivers.
The aim of this scoping study is to explore the current provision of paramedics in general practice, and describe what the intended benefits and unintended consequences of this workforce organisation might be.
The objectives of this study are to:
identify existing evidence on the effects of deploying paramedics in general practice;
characterise different models for deploying paramedics; and,
understand the hypotheses that underpin the models and explore the potential for unintended consequences for patients, staff, and the wider NHS.
Method
A mixed-methods scoping study was undertaken in three phases.
Phase 1: Literature review and survey
In order to map the existing deployment of paramedics in general practice, a systematically-searched scoping review of the literature including key national documents on the topic was completed. A web-based survey of paramedics, and staff working with them, in general practice was also carried out.
Literature review
Databases and search terms were agreed by the research team with the support of a subject specialist librarian (Table 1). Relevant articles and documents were identified by title and abstract, and a second reviewer repeated this process.
Survey
The survey contained 10 items and requested a mixture of categorical and free-text responses. It was developed in Qualtrics (version XM) by the study team in consultation with a wider stakeholder group and piloted with paramedics, GPs, practice managers, and commissioners. It was then administered to a convenience sample during June and July 2019 by the distribution of a web link as an open survey. The survey was cascaded by liaising with all local medical committees in England and distributed through a variety of CCGs, including national communication, and by utilising paramedic networks and social media. Consent to participate was obtained. There was no incentive offered for completion. Responses were anonymised and no identifiable data were collected.
Phase 2: Key informant (KI) meetings
Key informants (KIs) were met from two CCGs in the south west of England and professional bodies to identify existing theories about the intended outcomes of deploying paramedics in general practice. These meetings were also used to identify potential participants for phase 3. KIs were individuals employed within directly relevant organisations who had specific knowledge about, or experience of, paramedics working in general practice. KIs were identified by the study team using existing contacts and a snowball approach. The meetings between the researcher and each KI took place during April and May 2019 at a mutually agreed time and location. KIs gave written informed consent. Meetings lasted 30–40 minutes and were audiorecorded to supplement note-taking.
Phase 3: Stakeholder (SH) interviews
Direct enquiry with stakeholders (SHs)was used to examine the underlying assumptions about how different approaches to paramedic deployment were intended to work. A topic guide was developed by the research team in advance of the interviews and used to guide the interviews. The SHs were from two local CCGs in the south west of England. Participants were identified during phase 2 and were eligible if they were staff working in general practices with paramedics. The SHs were approached by email, and semi-structured face-to-face interviews were conducted by a researcher at a mutually agreed time and location. Participants gave written informed consent. Interviews lasted 30–50 minutes and were audiorecorded with an encrypted device, anonymised, and transcribed verbatim. Transcripts were analysed thematically by the primary researcher to examine the underlying assumptions about how different approaches to paramedic deployment are intended to work.20 Codes and categories were developed by the study team and 20% of the transcripts were double-coded by a second researcher.
Results
Phase 1
Literature review
Fourteen articles dating back to 1974 were included in the review (Table 1). The majority of articles are commentaries on the evolving role of paramedics and the training and skills required for paramedics to work in primary care settings. Recent commentaries support the role of paramedics in primary care settings and recognise the need to develop this further.2,4,5,8,11–13 However, there is no empirical evidence on the safety, clinical-, or cost-effectiveness of paramedics working in general practice. Searches of the grey literature returned descriptive documents, including job specifications, experiences of local initiatives, and discussions of paramedics’ skills. No key national documents were identified.
Survey
A total of 165 responses were received in a 4-week period. Eighty-seven (52.7%) responders specified the CCG in which they worked. Forty-five (23.6%) of 191 CCGs were specified; covering North of England, the Midlands, London, South East England, and South West England. One-third of the specifications were concentrated in South West England, with the remainder evenly spread across the other areas.
Seventy-five (45.5%) responders were paramedics, 32 (19.4%) were GPs, 40 (24.2%) were practice or business managers, and 18 (10.9%) were other staff such as nurses or pharmacists.
The majority of paramedics are employed directly by the GP practice. Others work across a primary care network, or are employed by a CCG, local ambulance service, or a community provider (Table 2). Ninety (54.5%) responders reported that paramedics had relevant post-registration qualifications. The reported qualifications were: clinical masters degree (MSc) (n = 17); diploma (n = 13); postgraduate certificate (n = 10); non-registered course (n = 18); working towards MSc or diploma (n = 13); did not specify, or referred to registration qualification (n = 19).
The tasks paramedics are undertaking are mostly same-day home visits (91.8%), followed by same-day clinics (74.7%), routine home visits (61.4%), and telephone triage (43.0%). A third of responders also reported that paramedics do pre-booked clinics (n = 53; 33.5%) and same-day telephone appointments (n = 56; 35.4%) (Table 2).
There was significant variation in reports on the types of condition and patient groups that paramedics are employed to see. This ranged from seeing all patients to focusing on acute presentations, older patients, or housebound patients. A total of 112 (67.9%) participants responded to a question about the types of patients that would not be seen by a paramedic. Of these, 137 (76%) reported one or more patient groups as exclusions. The most common exclusions were infants, pregnant women, and patients with mental health needs (Table 2).
The survey collected views on paramedics working in general practice. A total of 140 (84.8%) expressed a view; of these, 104 (74.3%) felt that paramedics working in general practice was a largely positive initiative (Figure 1).

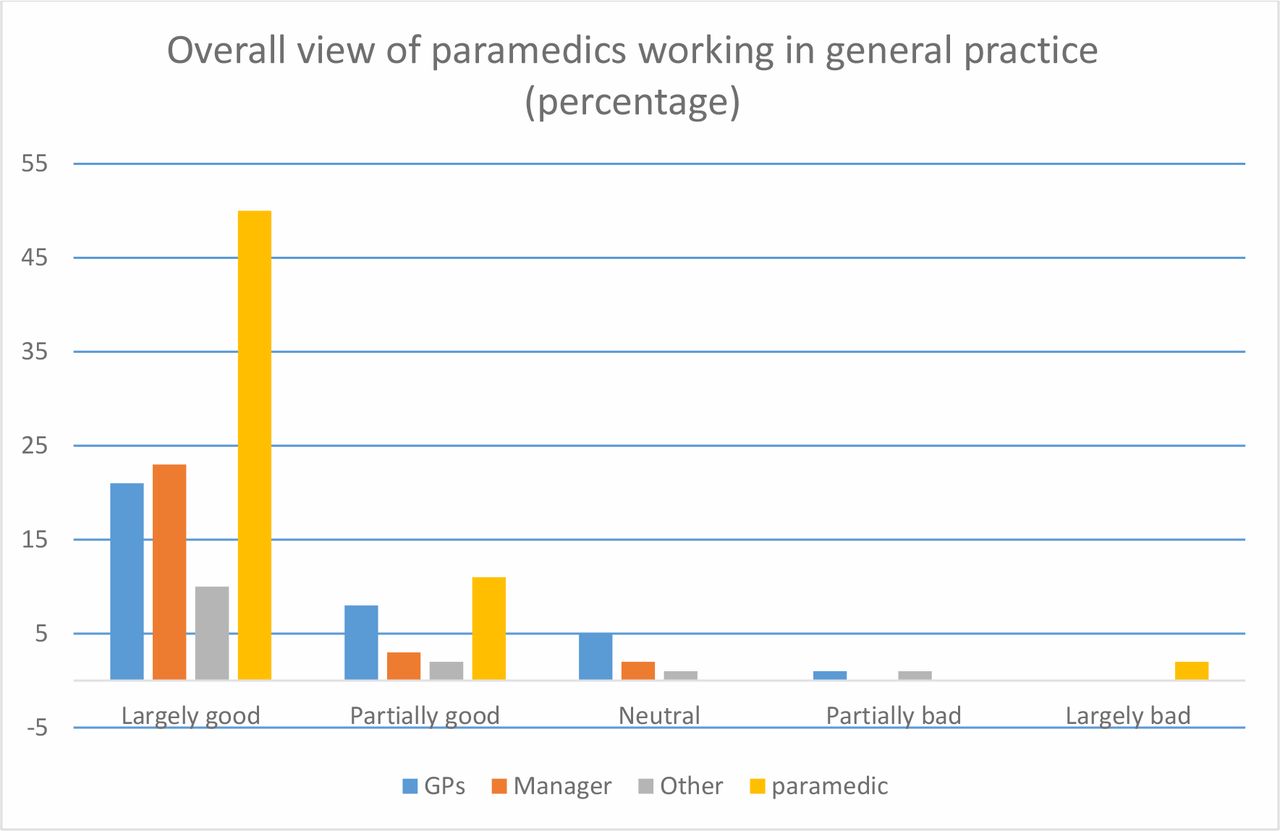{kind=link}
Missing data n = 25.
Phase 2: Key informant meetings
Nine KIs were approached and agreed to meet (Table 3). All KIs described their involvement in the planning, commissioning, or staff education of unplanned, urgent care, and primary care services within their localities. Some described roles and responsibilities specifically relating to workforce planning and development. The KIs were not aware of any CCG-led policy initiative to place or support paramedics in general practice. In their experiences, deployment of paramedics had been initiated at a practice level and evolved gradually over the previous 5 years. KIs spoke about the shortage of GPs and experienced advanced nurse practitioners, and acknowledged a need to deploy other healthcare professionals. Paramedics are recognised as clinicians with a skillset that is a valuable addition in primary care, rather than being used to replace GPs or deputise for them. No information is collected on paramedics working in GP practices by the CCG. KIs were less aware of the different nuanced models of paramedic deployment within primary care services. The advantages of paramedics working in primary care services were mostly envisaged as home visits and urgent cases being seen in a timelier manner.
KIs expressed concern that not all paramedics would be well-placed in general practice, depending on career stage and experience. However, they also identified the possibility that if more educated and experienced paramedics were to leave the ambulance service, the less experienced staff remaining could result in an increased conveyance rate to hospital. However, some KIs felt that if these paramedics were going to leave the ambulance service, employment in general practice is a way of retaining their skills within the NHS. There is a sense that paramedics are interested in portfolio careers and that the ambulance service is no longer seen as a 'job for life'. The rotational model, which is being piloted in England, was mentioned by some of the KIs as a model that could be replicated more widely.21
Phase 3: Stakeholder interviews
Ten SHs were approached and all agreed to be interviewed (Table 3). Codes were discussed by the study team and three themes emerged: the future of primary care; benefits and consequences for primary care; and professional challenges.
The future of primary care
The landscape of general practice is changing. There are not enough GPs; therefore, adaptive staff recruitment is required to meet the needs of patients. Although increasing GP numbers is seen as a priority, some clinical tasks can be undertaken by paramedics, which may save money:
'A very expensive, highly trained person doing every type of clinical role across the practice doesn’t make sense when you could employ people … who might be cheaper.' (SH6)
Conversely, this may not necessarily be seen as an effective use of resources:
' When I look at the home visits … we send the paramedic and then we send the paramedic the second time and then we send the GP the third time. So have we done more than we would've done normally and … I'm not convinced that we've actually saved anything. ' (SH3)
Continuity of care is a central tenet of general practice.22 In some cases, paramedics who undertake home visits can support this:
'[Paramedic] has been there for four years … [patients] get to know and trust the practitioners and they’re not just paramedics. ' (SH4)
Benefits and consequences for primary care
In general, paramedics are seen as a positive addition to the general practice team; reducing demand on GP time and ensuring more patients are seen sooner:
' So I think it benefits us but it also really benefits our patients because … [the paramedic] can say “Look I’ll be with you, you know, in half an hour” and we didn’t have that before. ' (SH2)
' For those patients where actually it's more of a social need to visit, then [the paramedic] are absolutely the right person who can spend half an hour where a GP can't. ' (SH3)
However, there are resource implications for the rest of the practice and other staff:
' GPs will say ”Well hang on, you know, I don’t want them spending forty, fifty minutes in the house … I want to see that level of value for money” … ' (SH5)
The tendency for paramedics to see low-complexity cases can result in GPs primarily seeing patients with multimorbidity, chronic illness, and, often, social complexities. This has the potential to impact on the job satisfaction and mental wellbeing of GPs:
' But if the paramedics see all of these “ easy stuff ” … you're left with only the really complicated stuff … I found that emotionally very hard work and draining. ' (SH4)
This may to some extent be explained by differences in clinical practice, as described by this paramedic:
' I guess that I'm able to give them a bit more time than a busy GP can and with that time I can use it to maybe do a fuller assessment … I have less knowledge so I need to check more things to make sure I'm not missing anything .' (SH1)
Nevertheless, if paramedics free up time, GPs can then complete other tasks more effectively, which reduces stress levels:
' If a GP has enough time, then what feels very stressful becomes more manageable. It is a huge psychological relief … ' (SH6)
Professional challenges
Paramedics in general practice are generally viewed in a positive light by participants in this study; however, the success of various models depends to some extent on how they are implemented and on the individuals involved:
' Perhaps all paramedics wouldn't be the same character you know, her character really she fitted in with our team really well and we’re very lucky. ' (SH2)
Some paramedics feel ‘out of their depth’ in general practice and do not stay in their primary care role for as long as planned:
' … good paramedic but his skills didn’t seem to transfer into general practice, so after about six months he decided that perhaps he's better off going back as a paramedic. ' (SH8)
There is limited agreement about the scope of practice for paramedics. One view is that ambulance service paramedics are best trained to deal with acute presentations:
' They're not very good at chronic disease management and that's essentially ‘cos they're paramedics … their job within the ambulance service is not the management of long-term diabetes or long-term COPD [chronic obstructive pulmonary disease]. ' (SH5)
An alternative view is that paramedics are well-equipped to deal with anything:
' We’re trained to see from the day you’re born, from the second you’re born to the second you die and we see everything in between that … different illnesses, chronic illnesses. ' (SH9)
Either way, effective supervision and support are essential:
' Some of the other paramedics have been forced into practice with no preparation and given timetabled slots with very little supervision and they're the ones that have found it difficult … ' (SH4)
However, a consequence of good support and supervision is the impact on GP time:
' We can have someone that we hope is going to take some load off us and for the first six months they may actually be a liability rather than a true asset and that's a challenge. ' (SH6)
Discussion
Summary
This scoping study aimed to explore the current provision of paramedics in general practice and describe what the intended benefits and unintended consequences of this workforce organisation might be. There is significant variation in the types of models adopted and disparity over a number of issues. The majority of models reported include home visits as a key feature. However, the type of patients seen and conditions treated vary significantly. On one hand, a perceived strength of a paramedic is that they have been trained to see all patients; on the other hand, paramedics are often excluded from seeing specific patient groups. An additional argument in support of deploying paramedics is that they will free up GP time; however, in some cases the amount of training, supervision, and support that is required may initially negate this. A third component to the debate is that paramedics cost less to employ; however, they may need substantially more time than GPs to assess and treat patients, and this assumption has not been tested empirically.
Strengths and limitations
These findings provide new information about the current provision of paramedics in general practice and what the intended benefits and unintended consequences of this workforce organisation might be. However, there are a number of limitations; the survey used a convenience sample and it is not possible to determine the response rate or whether the views expressed were representative of a wider group. The interviews were conducted within two neighbouring CCGs and this may limit the generalisability of the findings.
Comparison with existing literature
To the authors’ knowledge, there is no published evidence regarding the safety, clinical-, or cost-effectiveness of paramedics working in general practice.10 This study supports previous research asserting the need to understand and monitor the broader implications of changes in the general practice workforce,1,23,24 and offers some theories applicable to paramedics specifically.
Implications for research
The scale and significance of the issues discussed almost certainly varies according to local need, and further investigation is required to understand what works, and how, under differing circumstances. Research is needed to determine the effect of paramedics working in general practice on patient safety and experience, and to inform local and national decision making.
Notes
Funding
This study was funded by NHS Bristol, North Somerset and South Gloucestershire Clinical Commissioning Group (research capability funding). Reference number: 18/19-3SV.
Ethical approval
Approval for this study was obtained from the Health Research Authority and the University of the West of England Bristol Research Ethics Committee (reference number: HAS.19.02.134).
Provenance
Freely submitted; externally peer reviewed.
Acknowledgements
The authors would like to thank all those who participated in the survey, key informant meetings, and stakeholder interviews. In addition, the authors would like to thank the following academic collaborators for assisting with this work: Dr Helen Baxter, Knowledge Mobilisation Research Fellow, University of Bristol; Dr Alison Diaper, Senior Research Fellow, University of the West of England Bristol (UWE Bristol); Dr Andy Gibson, Associate Professor in Patient and Public Involvement, UWE Bristol; Justin Jagosh, Director of the Centre for Advancement in Realist Evaluation and Synthesis, University of Liverpool; Professor William Hollingworth, Professor of Health Economics, University of Bristol; Hazel Taylor, Statistician, Research Design Service South West; Sarah Todd, Programme Lead, Paramedic Education, UWE Bristol; Professor Nicola Walsh, Professor of Knowledge Mobilisation and Musculoskeletal Health, UWE Bristol.
Competing interests
The authors declare that no competing interests exist.
- Received November 5, 2019.
- Accepted December 9, 2019.
- Copyright © 2020, The Authors
This article is Open Access: CC BY license (https://creativecommons.org/licenses/by/4.0/)
References
In this issue








Jump to section
More in this TOC Section
Related Articles
Cited By...
