
Article Figures & Data
Figures
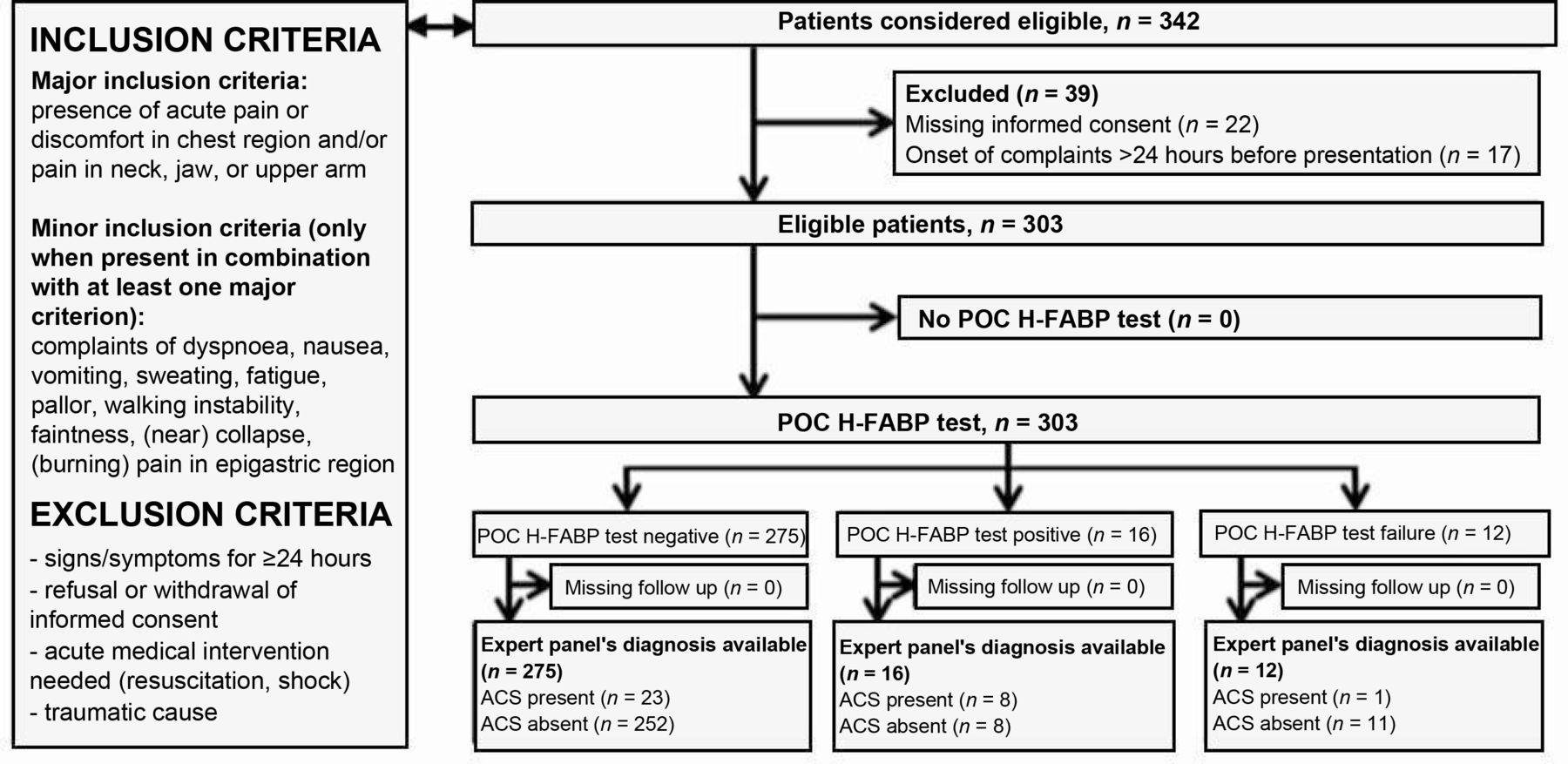
- Figure 1. Study flow chart showing inclusion and exclusion criteria, and eligible participants with numbers of main outcome (ACS).
ACS = acute coronary syndrome. H-FABP= heart-type fatty acid-binding protein. POC = point of care.
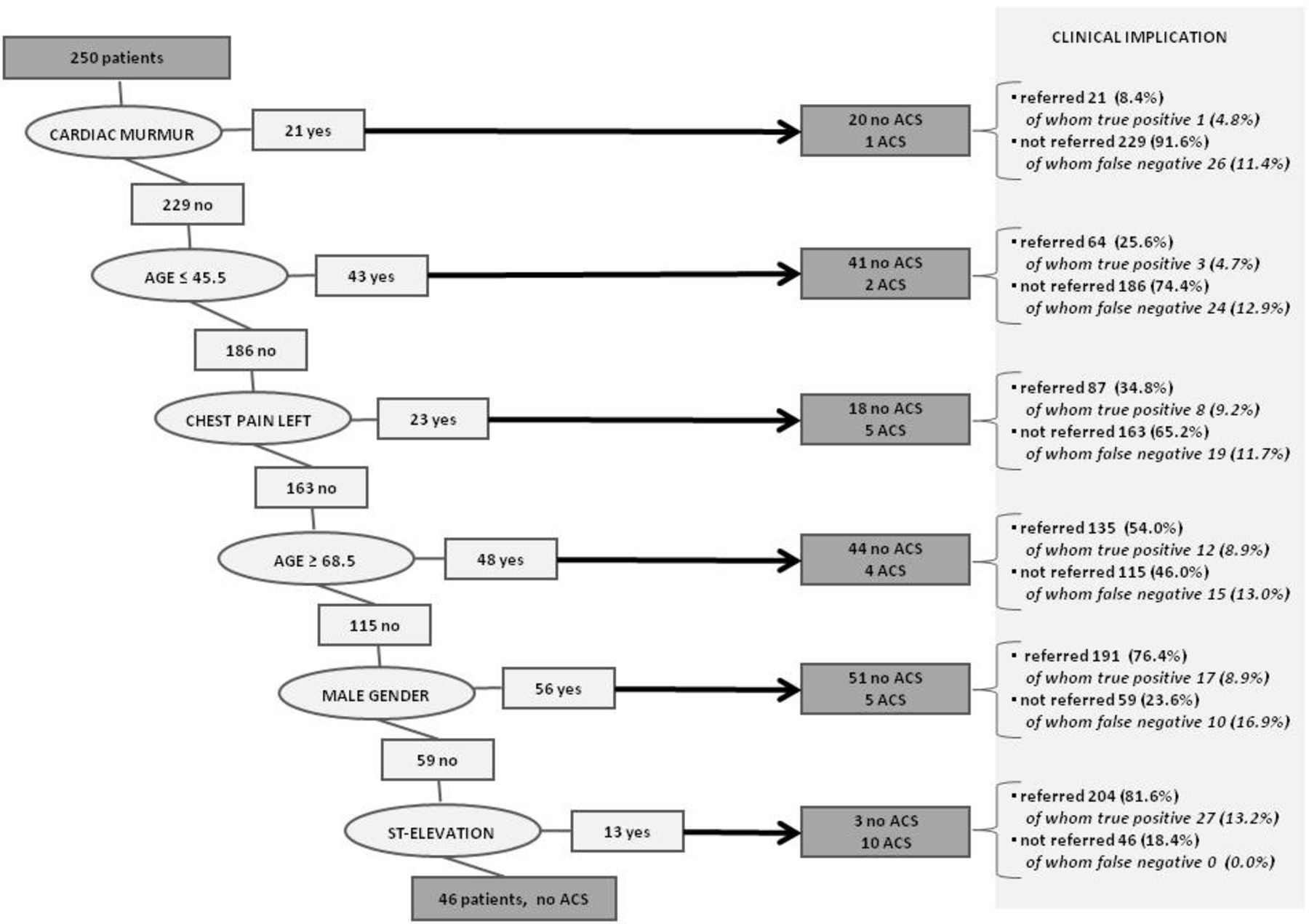
- Figure 2. Classification tree for acute coronary syndrome.
ACS = acute coronary syndrome.


{kind=link}
{kind=link}
Tables
Variable n (%) Remarks Sex Male 148 (48.8) – Female 155 (51.2) Age, years ≤30 15 (5.0) Mean age, years (range): 58.3 (17–100) 31–40 25 (8.3) 41–50 47 (15.5) 51–60 78 (25.7) 61–70 74 (24.4) 71–80 43 (14.2) >80 21 (6.9) Type of contact(missing data n = 1) Consultation, daytime, own GP 139 (46.0) 150 patients (49.7%) seen by their own GP during office hours, 152 patients (50.3%) seen by GP on call at OOH service Home visit, daytime, own GP 11 (3.6) Consultation, OOH service 146 (48.3) Home visit, OOH service 6 (2.0) History No DM2 or prior CVD 179 (59.1) – DM2 22 (7.3) Prior CVD 90 (29.7) DM2 and prior CVD 12 (4.0) Duration of complaints at presentation, hours(missing data n = 6) 0–1 32 (10.8) – 2–3 83 (27.9) 4–6 62 (20.9) 7–12 52 (17.5) 13–24 68 (22.9) eGFR, ml/min(missing data n = 49) ≤30 3 (1.2) – 31–60 42 (16.5) >60 09 (82.3) ECG performed(missing data n = 1) No 50 (16.6) – Yes, no abnormalities 152 (50.3) Yes, with abnormalities 100 (33.1) Referral policy No referral 167 (55.1) Overall referral percentage: 44.9% Overall direct referral percentage: 37.0% Overall referral percentage at later time: 7.9% Direct referral on presentation to cardiologist 107 (35.3) Direct referral on presentation, other 5 (1.7) Referral at later time during follow-up, cardiologist 20 (6.6) Referral at later time during follow-up, other 4 (1.3) Troponin available Troponin available (all patients) 267 (88.1) Troponin available (non-referred patients) 171 (87.2) Troponin available (referred patients) 96 (89.7) CVD = cardiovascular disease. DM2 = type 2 diabetes mellitus. ECG = electrocardiogram. eGFR = estimated glomerular filtration rate. OOH service = out-of-hours service.
Outcome: ACS or other life-threatening disease Outcome: ACS Outcome: AMI Outcome: NSTEMI Interval, onset complaints to presentation, hours 0– 24 0– 3 3– 24 0– 24 0– 3 3– 24 0– 24 0– 3 3– 24 0– 24 0– 3 3– 24 Patients, n 291a 106b 179b 291a 106b 179b 291a 106b 179b 291a 106b 179b Sens H-FABP POCT, % (95% CI) 25.7 (13.1 to 43.6) 8.3 (0.44 to 40.2) 36.4 (18.0 to 59.2) 25.8 (12.5 to 44.9) 9.1 (4.8 to 42.9) 36.8 (17.2 to 61.4) 26.9 (12.4 to 48.1) 10.0 (0.52 to 45.9) 40.0 (17.5 to 67.1) 18.9 (5.0 to 46.3) 0 (0 to48.3) 33.3 (9.0 to 69.1) Spec H-FABP POCT (95% CI) 97.3 (94.2 to 98.8) 98.9 (93.4 to 99.9) 96.2 (91.5 to 98.4) 96.9 (93.8 to 98.6) 98.9 (93.4 to 99.9) 95.6 (90.8 to 98.1) 96.6 (93.4 to 98.3) 99.0 (93.5 to 99.9) 95.1 (90.3 to 97.7) 95.3 (91.9 to 97.4) 98.0 (92.3 to 99.7) 93.5 (88.4 to 96.6) NPV H-FABP POCT, % (95% CI) 90.5 (86.3 to 93.6) 9.4 (81.5 to 94.3) 91.5 (85.9 to 95.1) 1.6 (87.6 to 94.5) 90.4 (82.6 to 95.0) 92.7 (87.4 to 96.0) 93.1 (89.2 to 95.7) 91.3 (83.8 to 95.7) 94.5 (89.6 to 97.3) 95.3 (91.9 to 97.4) 94.2 (87.4 to 97.6) 96.4 (91.9 to 98.5) PPV H-FABP PoCT, % (95% CI) 56.3 (30.6 to 79.2) 50.0 (26.7 to 97.3) 57.1 (29.6 to 81.2) 50.0 (25.5 to 74.5) 50.0 (26.7 to 97.3) 50.0 (24.0 to 76.0) 43.8 (20.8 to 69.4) 50.0 (26.7 to 97.3) 42.9 (18.8 to 70.4) 18.9 (5.0 to 46.3) 0 (0 to 80.2) 21.4 (5.7 to 51.2) Sensitivity, specificity, negative and positive predictive values of POC H-FABP for all patients, patients presenting within 3 hours of onset of complaints, and patients presenting 3–24 hours after onset of complaints for several outcomes, namely: (1) life-threatening disease (that is, composite of acute heart failure, pulmonary embolism, aortic dissection, acute death, ACS); (2) ACS (that is, UA, NSTEMI, STEMI); (3) AMI (that is, NSTEMI and STEMI); and (4) NSTEMI only.
a12 test failures among 303 included patients.
b In six cases, patients presented within 24 hours after onset of complaints; however, registration of duration of complaints was incomplete. These patients are not included in the tables representing subgroups of patients presenting with chest pain within 3 hours or 3–24 hours after onset of complaints.
ACS = acute coronary syndrome. AMI = acute myocardial infarction. CI = confidence intervals. H-FABP = heart-type fatty acid-binding protein. NPV = negative predictive value. NSTEMI = non-ST elevated myocardial infarction. POC = point of care. PPV = positive predictive value. Sens = sensitivity. Spec = specificity. STEMI = ST-elevated myocardial infarction. UA = unstable angina.
- Table 3. Sensitivity and specificity of possible clinical decision rules based on multivariable analyses of the study data (total patients with chest pain analysed, n = 303; total patients with ACS, n = 32 [10.6%]; total patients with AMI, n = 27 (8.9%])
Clinical judgment GP CDR variant 1 CDR variant 2 CDR variant 3 CDR variant 4 CDR variant 5 a,c CDR based on… ST-depressions / 1 1 / / / ST-elevations / 1 1 / / / Dyspnoea / 1 1 1 1 / Feeling of pressure chest / 1 1 1 1 / Absent lateral chest pain left / 1 1 1 1 – Age ≤45.5, ≥68.5 years / / / / / / Male sex / / / / / / Cardiac murmur / / / / / / POCT H-FABP result positive / 1 / 1 / / CDR and/or decision characteristics Maximum score / 6 5 4 3 / Considered negative if… GP did not refer ≤1 ≤1 ≤1 ≤1 / Patients with a negative versus positive score 191 negative, 112 positive 145 negative, 158 positive 147 negative, 156 positive 157 negative, 146 positive 161 negative, 142 positive 46 negative, 204 positive Rule-out characteristics Sens; NPV for ACS [95% CI] Sens 75.0 [56.2 to 87.9]; NPV 95.8 [91.6 to 98.0] Sens 87.5 [70.1 to 95.9]; NPV 97.2 [92.6 to 99.1] Sens 81.2 [63.0 to 92.1]; NPV 95.9 [90.9 to 98.3] Sens 78.1 [60.0 to 90.0]; NPV 95.5 [90.7 to 98.0] Sens 68.8 [49.9 to 83.3]; NPV 93.8 [88.6 to 96.8] Sens 100 [84.5 to 100]; NPV 100 [90.4 to 100] FNs for ACS, n (% of total) 8 (2.6) 4 (1.3) 6 (2.0) 7 (2.3) 10 (3.3) 0 (0.0) TNs for ACS, n (% of total) 183 (60.4) 141 (46.5) 141 (46.5) 150 (49.5) 151 (49.8) 46 (18.4) Sens; NPV for AMI [95% CI] Sens 70.4 [49.7 to 85.5]; NPV 95.8 [91.6 to 98.0] Sens 88.9 [69.7 to 97.1]; NPV 97.9 [93.6 to 99.5] Sens 81.5 [61.3 to 93.0]; NPV 96.6 [91.8 to 98.7] Sens 77.8 [57.3 to 90.6]; NPV 96.2 [91.5 to 98.4] Sens 66.7 [46.0 to 82.8]; NPV 94.4 [89.3 to 97.2] Sens 81.5 [61.3 to 93.0]; NPV 0 [0 to 53.7] Rule-in characteristics Spec; PPV for ACS [95% CI] Spec 67.5 [61.6 to 73.0]; PPV 21.4 [14.5 to 30.4] Spec 52.0 [45.9 to 58.1]; PPV 17.7 [12.3 to 24.8] Spec 52.0 [45.9 to 58.1]; PPV 16.7 [11.4 to 23.7] Spec 55.4 [49.2 to 61.3]; PPV 17.1 [11.6 to 24.4] Spec 55.7 [49.6 to 61.7]; PPV 15.5 [10.2 to 22.7] Spec 20.6 [15.6 to 26.7]; PPV 13.2 [9.1 to 18.8] FPs for ACS, n (% of total) 88 (29.0) 130 (42.9) 130 (42.9) 121 (39.9) 120 (39.6) 177 (70.8) TPs for ACS, n (% of total) 24 (7.9) 28 (9.2) 26 (8.6) 25 (8.3) 22 (7.3) 27 (10.8) Spec; PPV for AMI [95% CI] Spec 66.3 [60.4 to 71.8]; PPV 17.0 [10.8 to 25.5] Spec 51.4 [45.4 to 57.5]; PPV 15.2 [10.2 to 22.0] Spec 51.4 [45.4 to 57.5]; PPV 14.1 [9.2 to 20.8] Spec 54.7 (48.6 to 60.7]; PPV 14.4 [9.3 to 21.4] Spec 55.1 (49.0 to 61.0]; PPV 12.7 [7.9 to 19.6] Spec 0.0 (0.0 to 2.1]; PPV 9.0 [5.8 to 13.5] Rule in or outb Rule in, out ACS. Rule in, out AMI Rule in, out ACS. Rule in, out AMI Rule in, out ACS. Rule in, out AMI Rule in, out ACS. Rule in, out AMI Non-decisive Rule out ACS aDenominator in calculations for CDR variant 5 is 250 patients, since CART was initially performed in a subgroup of 53 patients and internally validated in a subgroup of the remaining 250 patients.
bA CDR is considered as possibly relevant for rule in when the pre-test probability (based on the prevalence in the study population) of presence of an AMI (8.9%), or ACS (10.6%), is below the lower margin of the 95% CI of the PPV of the CDR. A CDR is considered as potentially relevant for rule-out when the pre-test probability of absence of an AMI (91.1%), or ACS (89.4%), is below the lower margin of the 95% CI of the NPV.
cIn addition to the predicting signs and symptoms derived from CART for ACS, two other symptoms were added to CDR variant 5 for AMI: systolic blood pressure ≥149 mmHg and bradycardia (heart rate <60/min), based on the CART analysis with AMI as an outcome.
ACS = acute coronary syndrome. AMI = acute myocardial infarction. CI = confidence interval. FNs = false negatives. FPs = false positives. H-FABP = heart-type fatty acid-binding protein. NPV = negative predictive value. NSTEMI = non-ST elevated myocardial infarction. POCT = point of care test. PPV = positive predictive value. Sens = sensitivity. Spec = specificity. SBP = systolic blood pressure. TNs = true negatives. TPs = true positives.
In this issue








Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...
