
Article Figures & Data
Figures
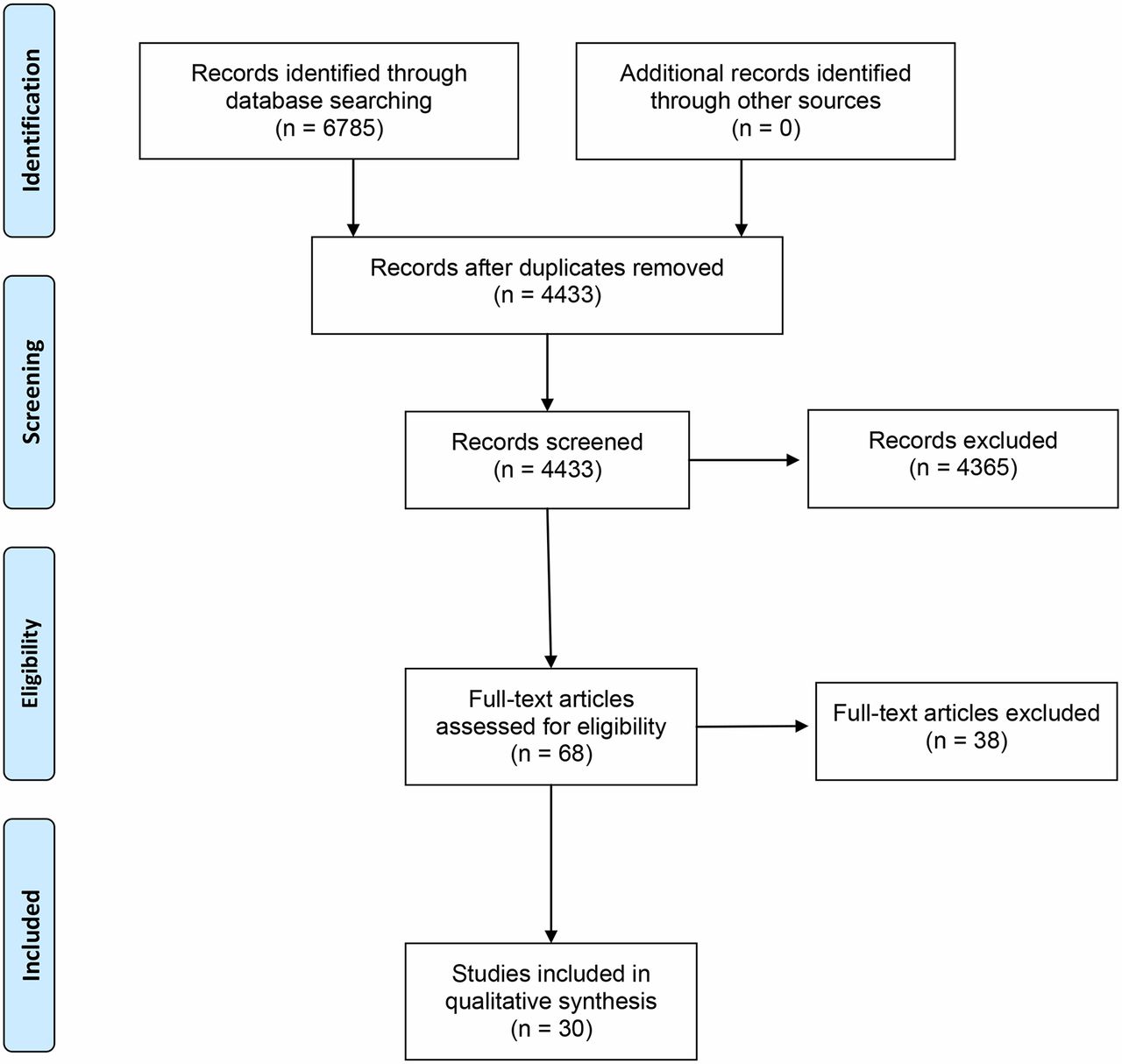
- Figure 1. PRISMA diagram.
{kind=link}
Tables
Class Patient symptoms I No limitation of physical activity. Ordinary physical activity does not cause undue fatigue, palpitation, dyspnoea (shortness of breath). II Slight limitation of physical activity. Comfortable at rest. Ordinary physical activity results in fatigue, palpitation, dyspnoea (shortness of breath). III Marked limitation of physical activity. Comfortable at rest. Less than ordinary activity causes fatigue, palpitation, or dyspnoea. IV Unable to carry on any physical activity without discomfort. Symptoms of heart failure at rest. If any physical activity is undertaken, discomfort increases. Class I Class II Class III Class IV Reference population, % 47 36 7 10 Extracted study, % 10 25 40 25 Extracted study with 10% deviation, % 0–20 15–35 30–50 15–35 Closeness of match, % >20 11–20 >20 11–20 Closeness of match, label Poor Fair Poor Fair Study ID Comparison Number of participants Primary outcome Follow-up, months AREA-CHF 2009 20 Canrenone
Placebo231
236Change in LV diastolic volume 12 BEST 2003 21 Bucindolol
Placebo114
112Death and heart failure hospitalisation composite 19 Borghi 2013 22 Ramipril
Zofenopril73
102Survival 73±14 CARNEBI 2013 23 Carvedilol
Bisoprolol
Nebivolol61
crossoverNYHA class, biochemistry, and physiological testing 6 (2 x 3 crossover) CELICARD 2000 24 Celiprolol
Placebo62
62Functional score — Goldman score 12 CHARM Added 2003 25 Candesartan
Placebo1011
1014Cardiovascular death or unplanned hospital admissions for worsening CHF 34 CHARM Alternative 2003 26 Candesartan
Placebo1273
1271Cardiovascular death or unplanned hospital admissions for worsening CHF 41 CIBIS 1994 27 Bisoprolol
Placebo320
321All-cause mortality 23 CIBIS 1999 28 Bisoprolol
Placebo1327
1320All-cause mortality 16 Cicoira 2002 29 Spironolactone
Placebo54
52Physiological or functional improvement 12 Cohn 2001 30 Valsartan
Placebo2511
2499All-cause mortality, and combined mortality and morbidity 23 Colucci 1996 31 Carvedilol
Placebo232
134Disease progression and death composite 12 COMET 2003 32 Carvedilol
Metoprolol1511
1518All-cause mortality 58 Dalla-Volta 1999 33 Delapril
Enalapril88
91Physiological or functional improvement 12 ELITE II 2000 34 Losartan
Captopril1578
1574All-cause mortality 18 Kum 2008 35 Add on Irbesartan
Placebo50
506MHW, Minnesota (QoL), peak exercise capacity on treadmill 12 Liu 2014 36 Metoprolol
Conventional therapy77
77NYHA class, LVESD, LVEDD, LVEF, 6-min walking distance, medication safety 6 MAIN CHF II 2014 37 Bisoprolol
Carvedilol21
14Clinical and functional status, mortality rate 8 MERIT-HF 1999 48 Metoprolol CR
Placebo1990
2001All-cause mortality 12 Munich 1991 38 Captopril
Placebo83
87Cardiovascular-cause mortality 33 Pitt 1999 9 Spironolactone
Placebo822
841All-cause mortality 24 Riegger 1999 39 Candesartan 4 mg
Candesartan 8 mg
Candesartan 16 mg
Placebo211
208
212
213Increase in exercise tolerance, reduction in NYHA class 3 SENIORS 2005 40 Nevovitol
Placebo1067
1061All-cause mortality and time to first CVD admission 21 SOLVD 1991 41 Enalapril
Placebo1285
1284Clinical and functional status, mortality rate 41.4 SOLVD 1992 42 Enalapril
Placebo2111
2117Clinical and functional status, mortality rate 37.4 Sturm 2000 43 Atenolol
Placebo51
49Worsening heart failure or death 24 US Carvedilol 2001 44 Carvedilol
PlaceboBlack: 127
Not Black: 569
Black: 90
Not Black: 308Ethnicity (self-reported), ejection fraction, clinical status, and major clinical events 15 Yodfat 1991 45 Captopril
Placebo41
43Functional status 3 Zannad 1998 46 Fosinopril
Placebo122
132Cardiovascular mortality and event-free survival 12 Zannad 2011 47 Eplenerone
Placebo1364
1373Cardiovascular mortality and event-free survival 21 6MHW = 6-minute hall walk. CHF = congestive heart failure. CVD = cardiovascular disease. LV = left ventricular. LVEDD = left ventricular end-diastolic diameter. LVEF = left ventricular ejection fraction. LVESD = left ventricular end-systolic diameter. NYHA = New York Heart Association. QOL = quality of life.
Characteristic Total (n = 72), n (%) Mean age, years (SD) 69 (9) Female 14 (19) Male 58 (81) Ever smoked 50 (69) Non-white 2 (3) Any electrocardiogram abnormality 2 (3) Mean height, metres (SD) 1.71 (0.09) Mean weight, kg (SD) 80.8 (14.6) Mean heart rate, beats per min (SD) 77.3 (17.8) Mean forced expiratory volume at 1 second, litres (SD) 2.11 (0.76) Mean forced vital capacity, litres (SD) 2.55 (0.85) Mean systolic blood pressure, mmHg (SD) 148.4 (21.1) Mean diastolic blood pressure, mmHg (SD) 87.1 (12.3) New York Heart Association class I 34 (47) II 26 (36) III 5 (7) IV 7 (10) History Myocardial ischaemia 38 (53) Angina 26 (36) Hypertension 28 (39) Diabetes 11 (15) Family myocardial ischaemia (age <65 years) 25 (35) Medication taken ACE inhibitors 19 (26) Diuretics 26 (36) Beta-blockers 9 (13) Calcium antagonists 15 (21) Aspirin 38 (53) Digoxin 5 (7) SD = standard deviation.
NYHA class 5 Heart failure RCTs N Ia, % IIb, % IIIc, % IVd, % SOLVD 1992 4228 11–20 <10 <10 <10 Munich 1991 170 11–20 11–20 11–20 <10 Borghi 2013 175 11–20 11–20 11–20 <10 US Carvedilol 1996 1094 >20 <10 >20 <10 Liu 2014 154 >20 <10 >20 <10 CHARM Added 2003 2548 >20 <10 >20 <10 MERIT-HF 1999 3991 >20 <10 >20 <10 Zannad 1998 254 >20 >20 <10 <10 CELICARD 2000 124 >20 11–20 >20 <10 CHARM Alternative 2003 2028 >20 11–20 >20 <10 SENIORS 2005 2128 >20 11–20 >20 <10 SOLVD 1991 2569 >20 11–20 >20 <10 COMET 2003 3029 >20 11–20 >20 <10 Cicoira 2002 106 e
e
e
e
CARNEBI 2013 183 >20 >20 <10 >20 MAIN CHF II 2014 59 >20 >20 <10 >20 Colucci 1996 366 >20 >20 <10 >20 Zannad 2011 2737 >20 >20 >20 <10 Sturm 2000 100 >20 >20 >20 <10 Cohn 2001 5010 >20 >20 >20 <10 CIBIS 1994 641 >20 >20 >20 <10 CIBIS 1999 2647 >20 >20 >20 <10 ELITE II 2000 3152 >20 11–20 >20 >20 Kum 2008 100 >20 11–20 >20 >20 Rieger 1999 844 >20 >20 11–20 >20 BEST 2003 226 >20 >20 >20 >20 Dalla-Volta 1999 179 >20 >20 >20 >20 AREA-CHF 2009 382 >20 >20 >20 >20 Pitt 1999 1663 >20 >20 >20 >20 Yodfat 1991 84 e e
e
e
a47% of reference population. b36% of reference poulation. c7% of reference population. d10% of reference population. eInsufficient information to calculate deviation. RCT = randomised controlled trial. NYHA = New York Heart Association.
In this issue
Are patients in heart failure trials representative of primary care populations? A systematic review








Jump to section
More in this TOC Section
Related Articles
Cited By...
Intended for Healthcare Professionals
