Article Text

Abstract
Objective Synthesise evidence about the impact of family medicine/general practice (FM) clerkships on undergraduate medical students, teaching general/family practitioners (FPs) and/or their patients.
Data sources Medline, ERIC, PsycINFO, EMBASE and Web of Knowledge searched from 21 November to 17 December 2013. Primary, empirical, quantitative or qualitative studies, since 1990, with abstracts included. No country restrictions. Full text languages: English, French, Spanish, German, Dutch or Italian.
Review methods Independent selection and data extraction by two authors using predefined data extraction fields, including Kirkpatrick’s levels for educational intervention outcomes, study quality indicators and Best Evidence Medical Education (BEME) strength of findings’ grades. Descriptive narrative synthesis applied.
Results Sixty-four included articles: impact on students (48), teaching FPs (12) and patients (8). Sample sizes: 16-1095 students, 3-146 FPs and 94-2550 patients. Twenty-six studies evaluated at Kirkpatrick level 1, 26 at level 2 and 6 at level 3. Only one study achieved BEME’s grade 5. The majority was assessed as grade 4 (27) and 3 (33). Students reported satisfaction with content and process of teaching as well as learning in FM clerkships. They enhanced previous learning, and provided unique learning on dealing with common acute and chronic conditions, health maintenance, disease prevention, communication and problem-solving skills. Students’ attitudes towards FM were improved, but new or enhanced interest in FM careers did not persist without change after graduation. Teaching FPs reported increased job satisfaction and stimulation for professional development, but also increased workload and less productivity, depending on the setting. Overall, student’s presence and participation did not have a negative impact on patients.
Conclusions Research quality on the impact of FM clerkships is still limited, yet across different settings and countries, positive impact is reported on students, FPs and patients. Future studies should involve different stakeholders, medical schools and countries, and use standardised and validated evaluation tools.
- MEDICAL EDUCATION & TRAINING
- Family Medicine
- Clerkship
- Impact
- Undergraduate medical education
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Systematic review of 64 studies on the impact of family medicine/general practice clerkships on medical students, teaching general/family practitioners and/or their patients, from 1990 to 2013, without country limitations.
Comprehensive search strategy using the major databases for medical and educational research and following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Studies assessed for research quality, Kirkpatrick’s levels of educational outcomes and Best Evidence Medical Education (BEME)’s grades of strength of findings.
Lack of meta-analysis due to variety of study designs, evaluation tools and outcomes and the reported results.
Despite the comprehensive search strategy, due to full-text language and accessibility limitations, other studies published in this research area may have been missed.
Introduction
In the past few decades, family medicine/general practice (hereafter FM) has developed into a clinical and academic discipline aiming to provide comprehensive and quality patient care, and to contribute to medical research and education.1–4 As a primary care discipline with an untapped potential for contribution to medical education, FM has played an important role in the trend of the past few decades to orient medical school curricula toward community-based health services alongside those traditionally hospital-based.5–7 In light of the increasing need to address complex and multiple chronic conditions in ageing societies, and the recognition of the complementary roles of hospital and primary care, current recommendations call for more exposure of medical students to primary care and FM as its core medical specialty.8–10
The contribution of FM in the undergraduate medical curriculum is multifaceted, reflecting the broadness and comprehensiveness of the specialty itself. In the junior/preclinical years, FM may provide early exposure to patients, introducing students to the doctor–patient relationship and the influence of illness in families, as well as teaching on communication and clinical skills. During the senior/clinical years, the main contribution is teaching about the specialty of FM by either block or longitudinal clinical experiences (clerkships) or providing shared experiences of primary and secondary/tertiary care with other specialties.6 ,11–14
Yet, the level of involvement and contribution of FM in undergraduate medical education varies in different countries, depending on its scope of practice and role in the healthcare system, as well as its academic status. The EURACT (European Academy of Teachers in General Practice and Family Medicine) has recently mapped the availability of FM clerkships in all European schools through a survey of 259/400 medical schools in 39 European countries, revealing variability between European regions regarding the availability, length and scope of FM clerkships.15 Fifty medical schools, mostly in Southern and Eastern Europe, reported either a lack of or only very brief FM clerkships.15
Previous reviews on ambulatory care teaching and learning experiences in North America that included studies on both undergraduate and postgraduate programmes in internal medicine, FM, paediatrics or other ambulatory care specialties until 1999, have confirmed their positive educational contribution, yet called for further and more rigorous research, especially on learning outcomes.16–18 Recent reviews on longitudinal integrated clerkships, placements of students in rural and underserved areas, and mapping the contribution of undergraduate ambulatory education to the Canadian recommendations for undergraduate medical education have included learning experiences in FM clerkships.19–21 Yet to our knowledge, no published systematic review so far has focused specifically on the impact of FM clerkships and extended beyond North America.
We perceive there is a need for such a systematic review, in light of the previously reported valuable educational opportunities of ambulatory undergraduate education in North America and the current limited availability of FM clerkships in some parts of Europe and internationally.1 ,15
The aim of this review is to search, analyse and synthesise evidence about the impact of FM clerkships on learning outcomes of undergraduate medical students, general/family practitioners (hereafter FPs) who host the students in their practices, as well as on their patients.
Methods
This systematic review was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.22
Selection criteria
The included papers involved undergraduate medical students, teaching FPs or patients in FM clerkships, as participants. FM clerkships were defined as structured periods of clinical experiences in FM to learn about the FM specialty, during which students work with patients, under supervision of a preceptor/tutor, and attend didactic sessions delivered by FM faculty.23 These clerkships might be either a block of several weeks or longitudinal experiences spread throughout the whole semester/year. The outcomes of studies included in this review were the impact of FM clerkships on the education of the participating students, the work of the teaching FPs, and/or on their patients. The adapted Kirkpatrick levels for educational intervention outcomes were used to assess the impact of the FM clerkship on the education of students.24 Kirkpatrick's levels 1 and 2 consider students’ views on the learning experience of the FM clerkship (1), changes in attitudes towards FM (2A), and knowledge and/or skills (2B), as a result of the clerkship. Level 3 involves transfer of learning to practice, while level 4 considers changes in organisational practice (4A) or benefits to patients (4B) as a direct result of the learning during the FM clerkship.
The review’s selection criteria were discussed and agreed among three of the reviewers (ET, RR and NM; table 1).
Inclusion and exclusion criteria
All empirical quantitative or qualitative studies from 1990 onward, with available abstracts and primary data on the impact of FM clerkships on medical students, teaching GP/FPs and/or patients, were included. No restrictions were applied on country, but full text languages were limited to English, French, Spanish, German, Dutch or Italian (languages spoken by reviewers).
Studies that focused on some other specific features of teaching and learning in FM such as rural versus urban setting, introduction of specific teaching or assessment methods, as well as those assessing students’ clinical exposure during preclinical/junior years, were excluded.
Search strategy
The essential concepts used for the search strategy were: general practice/FM/primary care (discipline/practice and practitioners) and clinical clerkships/attachments/rotations/placements/clinical experiences/preceptorships. Medline (via Ovid), ERIC, PsycINFO, EMBASE and Web of Knowledge were searched from 21 November to 17 December 2013. The search syntax used a combination of terms for key concepts adapted to each database (see online supplementary appendix). Additional relevant studies were identified based on expert knowledge of the reviewers.
Study selection
Two reviewers (ET and RR or NRM) independently screened titles and abstracts selecting those that met inclusion criteria. The full-texts of the selected articles were independently assessed against the search criteria by two reviewers (ET and RR or NRM). In case of disagreement or uncertainty, the reviewers discussed and when necessary the opinion of a third reviewer was considered for the final decision.
Data extraction and analysis
One of the reviewers (ET) extracted data from each full-text article using a purpose-designed data extraction form based on the Best Evidence Medical Education (BEME) coding form.25 ,26 A second reviewer (RR, NRM or KH) checked the extracted data. In case of disagreement, the opinion of a third reviewer was used for the final decision.
Extracted data focused on the clerkship (country, setting, location in the curriculum, duration, aims and objectives) and study methodology (design, data sources, population and measured outcomes). The methodology rigour of studies was evaluated with a checklist adapted from a previous medical education systematic review.26 The strength of findings for each study was scored on the BEME scale of 1–5:25
Grade 1: No clear conclusions can be drawn; not significant
Grade 2: Results ambiguous, but there appears to be a trend
Grade 3: Conclusions can probably be based on the results
Grade 4: Results are clear and very likely to be true
Grade 5: Results are unequivocal.
Owing to the variety of measured outcomes, methods and tools, methodological quality and reported statistics of the included studies, meta-analysis was not possible. Descriptive narrative synthesis was used for the analysis and synthesis of the findings.27 The synthesis will report on the types of FM clerkships in terms of duration, location in curriculum, setting and learning aims and objectives; studies’ countries and year of publication, evaluation methods, Kirkpatrick outcome evaluation level, methodological quality and the main findings related to the impact of FM clerkships on medical students, teaching FPs and/or their patients.
Results
Search results
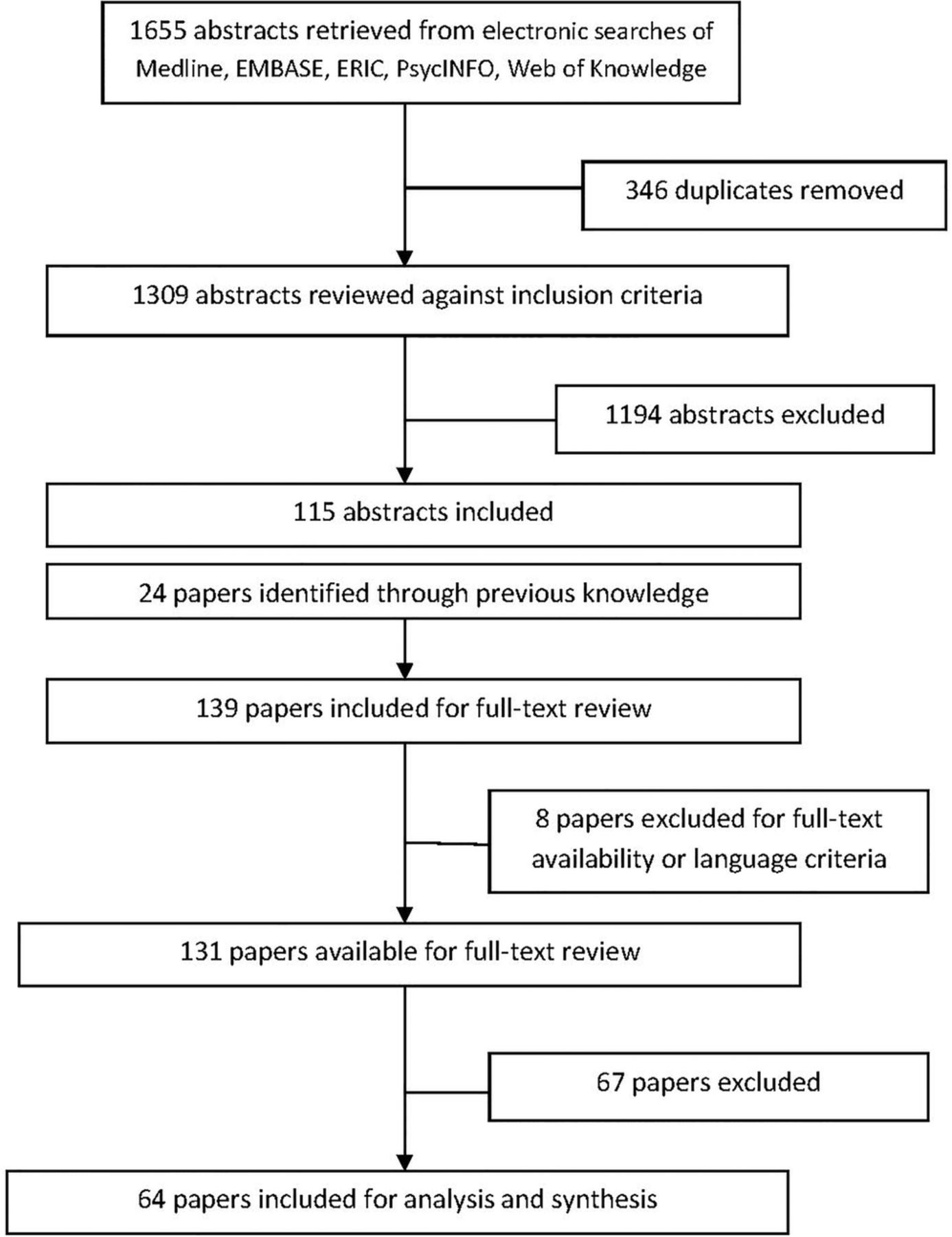
The search strategy identified 1655 papers, which were entered in Endnote X6 (figure 1). After de-duplication and screening of titles and abstracts, 1540 papers were excluded mainly because they focused on other aspects of FM involvement in medical education, non-educational aspects of FM or postgraduate FM. Four papers selected for full-text review were not available even after using inter-university library exchange, while four others were available only in Chinese, Norwegian or Hebrew.

{kind=link}
Flow diagram of the process of search and selection of the papers.
After full-text review, 64 papers were selected for data extraction and analysis. The main reasons for exclusion at this stage were clerkship not focused on the discipline of FM, population being preclinical or not clearly clinical students or the clerkship’s impact was not the study’s main focus.
Study characteristics
Out of the 64 included studies, 56% were published from 1990 to 2000, and the majority were from the USA (30 studies) and Europe (21 studies; table 2).
Distribution of reviewed studies by country and publishing year intervals
Forty-eight studies reported the impact of FM clerkships on students, 12 on teaching FPs and their practices and 8 on patients involved in FM clerkship teaching. Three studies had a mixed target population of students, FPs and/or patients.28–30
Thirteen studies were non-randomised controlled studies and 12 were pre–post (uncontrolled) studies (table 3). The sample size ranged from 16 to 1095 students, 3 to 146 teaching FPs and 94 to 2550 patients. The methods used to evaluate the impact of FM clerkships were mostly questionnaire surveys (36 studies) and patient encounter forms/logs of students or coding/billing forms of FPs (13 studies) (table 3).
Distribution of reviewed study by design and data sources
Clerkship format
FM clerkships varied considerably in duration and setting. The duration ranged from 2 to 12 weeks, with one study reporting on a year-long longitudinal clerkship,31 while in eight papers the duration of the clerkship was not clearly stated. The setting was mainly mixed (urban and rural) for 23 studies, urban for 9 and rural for 1 study,32 while for 31 studies the setting was not clearly stated. The clerkships were mainly obligatory (56 studies) and took place in year 3 (27 studies in USA), years 4–5 (10 studies) or years 5–6 (22 studies), while three studies did not clearly report the curriculum year of the clerkship. The aim and goals of the clerkships were reported only in nine papers33–41 and included: providing exposure to the role of FM and primary care as a medical practice setting and assisting students in making their career decision; refining and consolidating history taking and physical examination skills in the FM setting with a special emphasis on communication skills, and the doctor–patient relationship; dealing with most common medical problems in FM and its specific management principles such as undifferentiated problems, home visits, referrals, etc; learning about business/organisational aspects of the medical practice and the role of team-work.
Kirkpatrick outcome levels
Table 4 summarises the proportion of studies that assessed the impact of FM clerkships at each Kirkpatrick outcome level.
Distribution of reviewed studies by Kirkpatrick outcome levels and strength of findings
Twenty-six (41%) studies reported students’ views on the quality of the clerkship (level 1), while the rest of the studies reported changes in attitudes, knowledge/skills or behaviours (levels 2 and 3). Although none of the reviewed studies reported the evaluation of the transfer of students’ learning during FM clerkships into their workplace, we included, under Kirkpatrick level 3, six studies that followed up and reported the entrance of graduates in FM specialty training considering it as an application of their learning about FM during the clerkship. None of the reviewed studies reported effects on the system/organisation or patient care outcomes as a direct result of the knowledge, skills and attitudes gained by students in the FM clerkship (level 4).
Methodological quality
Table 4 reports the number of studies in each of the five grades of strength of findings. The majority of studies were grade 3 (52%) or 4 (42%). Only one study was graded as 5 (unequivocal results).42 The quality criteria that were most commonly unclear or not met included accounting for multiple variables/factors, generalisability of conclusions, addressing relevant ethical issues as well as using data from more than one source.
Synthesis of findings on the impact of FM clerkships
Impact on students
Table 5 provides information about each study that evaluated the impact of the FM clerkship on students for each Kirkpatrick outcome level.
Studies reporting impact of FM clerkships on students according to Kirkpatrick outcome levels
Satisfaction with the teaching and learning experience
Twenty-six studies reported students’ evaluation of the quality of the FM clerkship in several countries such as the USA,28 ,38 ,43–47 the UK,39 ,48–51 Germany,52 ,53 Austria,30 ,54 Israel,55 ,56 Slovenia,40 ,57 Ireland,58 Pakistan,59 Sweden,34 Saudi Arabia,36 South Africa60 and Australia.61 Nineteen (73%) studies used evaluation questionnaires,30 ,34 ,36 ,38 ,39 ,40 ,46 ,47 ,49 ,50 ,52–57 ,59–61 two interviews39 ,51 and three focus groups,39 ,56 ,60 either alone or in combination with questionnaires, while six studies used students’ patient encounter or activity logs.28 ,43–45 ,48 ,58 The questionnaires used Likert or similar rating scales to assess satisfaction of students and most of them included open-ended questions. They were self-developed based on previous literature, local experience and clerkship’s learning objectives. Only two studies reported some reliability and validity measures for their questionnaires/patient encounter or activity logs,34 ,45 while one study used an internationally validated questionnaire for measuring the educational environment.53 Almost all questionnaires were handed out at the end of the clerkship, except for six studies that evaluated both at pre-clerkship and post-clerkship.36 ,40 ,49 ,50 ,52 ,59
Students rated their overall satisfaction with the FM clerkship as very high.30 ,34 ,36 ,38–40 ,47 ,49 ,52–56 ,59–61 In different countries with different levels of FM development, students repeatedly reported on the high quality of teaching and the variety of learning experiences during FM clerkships.28 ,36 ,39 ,43–45 ,48 ,50–52 ,56–59 ,61 ,62
Students were satisfied with the quality of the teaching setting and their relationship with FPs as they were enthusiastic, welcoming and friendly, willing to answer questions and set aside time to discuss with them.28 ,30 ,34 ,36 ,39 ,48 ,54 ,55 ,57 ,61
The most commonly cited satisfactory aspects of FM clerkships were exposure to a variety of health problems including acute and chronic problems, preventive and continuity visits,39 ,44 ,45 ,51 ,58 ,60 ,61 dealing with undifferentiated symptoms and managing common health problems,36 ,50 ,52 ,56 ,59–61 making holistic assessment of patients considering the psychosocial aspects of the disease,39 ,50 ,51 ,56 ,60 learning communication and physical examination skills,39 ,45 ,50–52 ,56 ,59 ,60 as well as about the organisation of primary care, its team and the role of FPs.36 ,39 ,56 ,57 ,60 Learning experiences in FM clerkships were reported as complementary and reinforcing to those in ambulatory care internal medicine and paediatrics.43 ,45
Change in attitudes to FM and career choices
Sixteen studies evaluated the impact of the clerkship on students’ attitudes towards FM as a specialty and their career choices.32 ,33 ,40 ,42 ,47 ,49 ,50 ,59 ,63–70 Attitudes were assessed either through attitudinal statements with Likert scales,40 ,47 ,63 ,64 focus groups33 ,65 and/or using interest/intention for a future career in FM as a proxy for attitudes toward FM.32 ,40 ,47 ,49 ,50 ,59 ,63–67 Nine studies evaluated both at pre-clerkship and post-clerkship32 ,40 ,47 ,49 ,50 ,59 ,63 ,64 ,66 with three of them at 1 year after graduation49 or at the time of specialty selection.32 ,47 Three studies looked only at post-clerkship attitudes,33 ,65 ,67 but one of them followed up students at 18–26 months after clerkship.67 One study also looked at the pre–post clerkship career intentions/preferences changes in internal medicine and surgery clerkships.64
Studies reported from countries with a well-established clinical and academic discipline of FM such as the Netherlands, UK, Ireland and the USA,32 ,47 ,49 ,50 ,58 ,64 ,65 as well as from countries with a mostly hospital-based/oriented healthcare system with no clearly defined complementary roles between specialists and generalists, such as Pakistan, Hong-Kong, Turkey and Germany.33 ,59 ,63 ,66 ,67 Although all quantitative studies except for one67 report inferential statistics, only two performed some multivariable analysis on career intentions/choices including gender and attitudes.63 ,64
Almost all studies report that the FM clerkship had a positive effect on improving students’ attitudes toward FM.33 ,40 ,47 ,50 ,63 ,65 The clerkship experience helped in counteracting the negative FM stereotypes as low-status and intellectually unchallenging.33 ,63 ,65 Yet, this attitude change does not necessarily translate into increase of interest in a future FM career,40 ,63 ,67 or increases interest only among those already interested in FM or not sure yet about their future career interests.50 ,59 The perceived likelihood of choosing the clerkship’s specialty increased in almost similar levels (around 30%) after FM, internal medicine and surgery clerkships, but the FM and surgery clerkships caused a shift of career preference motives from external (status, income and career prospects) to internal (variety of work and patients), suggesting a change of views regarding these specialties.64 In Turkey, even though there was no significant difference in attitudes towards FM after the clerkship, there was still a statistically significant increase in ranking of FM as a career choice.66
Increased interest in a FM career after the clerkship decreases over time49 and only a minority of those with an increased interest enter the FM specialty training.47 Only in one study of a rural US FM clerkship, did the majority of those who had a positive shift towards an interest in FM career enter FM specialty training.32
In the USA, medical schools with a required third year FM clerkship had higher numbers of graduates entering FM specialty training programmes compared to schools without a required FM clerkship.68–70 Even after adjusting for students’ sociodemographic background and specialty preferences, the educational value of the FM clerkship was an independent predictor of entering FM specialty training (OR 2.9 95% CI 1.1 to 7.3 p=0.024).42
Change in knowledge and/or skills
Thirteen studies report impact of the FM clerkship on students’ knowledge and/or skills. The majority are from the USA (10 studies),35 ,37 ,71–78 with only two studies from Europe (Slovenia and Austria)54 ,57 and one from United Arab Emirates.41 Two studies assessed with written examinations,71 ,73 one with objective structured clinical examination (OSCE),41 and one with tutor/preceptor evaluation forms.57 The rest of the studies used rating of students’ self-perceived competence/confidence.35 ,37 ,54 ,72 ,74–78 Only six studies used either a non-randomised controlled71 ,73 or the pre–post clerkship comparative35 ,37 ,41 ,78 design to adjust for academic performance and learning before the FM clerkship.
Areas with improved knowledge or skills attributed to the FM clerkship were preventive medicine for different age groups, clinical decision-making and problem solving, management of common health problems, focused patient evaluation, communication and cooperation with the practice team, record keeping, prescribing, referral systems, dealing with ethical problems, as well as a few practical procedures.35 ,41 ,57 ,71 ,78 In a US clerkship, students’ perceived competence/confidence was higher than average for dealing with the 10 most frequent ear-nose-throat and psychiatric diagnoses, but lower for obstetrics-gynaecology and muscular-skeletal diagnoses.74–77 The National Board of Medical Examiners (NBME II) scores of students who had taken the FM clerkship and those who had not (control group with similar scores in NBME I) had no statistically significant difference for the medicine and surgery parts of the examination. Students who had a FM clerkship scored significantly higher only in the public health items of NBME II.71
The increase in knowledge/skills due to the FM clerkship measured by improved multiple choice questions examination or OSCE scores remained even after prior experience in other specialties’ clerkships.41 ,73 Depending on the timing of the FM clerkship in the curriculum, there was self-reported gain in knowledge and skills between pre–post clerkship for 25/26 core medical conditions if the clerkship took place before and 16/26 if it took place after the internal medicine, obstetrics-gynaecology and psychiatrics clerkships.37 Yet, acquiring knowledge about undifferentiated and commonly seen problems, health promotion, disease prevention and patient education, importance of family dynamics in patient care and business aspects of medical practice, were reported as gains even when the FM clerkship was taken after all other clerkships.37
Impact on teaching FPs
The impact on teaching FPs was reported by 12 studies from the USA,28 ,46 ,62 ,79–83 Austria,29 ,30 the UK84 and Australia85 (table 6).
Studies reporting the impact of FM clerkships on teaching FPs and their patients
Questionnaires, interviews and observations as well as coding/billing or patient encounter forms were used to collect data. Only three studies used a comparative non-randomised approach where clinical sessions with students were compared to those without students,79 ,80 or teaching FPs were compared to non-teaching colleagues.83
Teaching FPs are overall satisfied with their role as they report excitement from teaching and enthusiasm from interacting with students and investing in their development.30 ,62 ,81 ,82 ,85 They also report learning while teaching as interaction with students and their questions provide stimulation to keep up to date with developments of medical knowledge, as well as encourage reflective practice and have a positive effect on their professional development.29 ,62 ,81 ,84 ,85 Involvement in teaching students also provided an opportunity to upgrade clinical skills and develop teaching skills and improved relationship with other staff and team development, as well as their professional status and relationship with patients.29 ,81 ,84
The main disadvantages reported by teaching FPs were slowed down patient flow and increased working hours.29 ,46 ,62 ,81 ,82 ,85 Data on length of workday and productivity (number of patients seen) when a student is present are based mainly on self-report, although two studies observed and timed consultations of FPs with students,62 ,83 and two studies analysed patient encounter or billing/coding forms.79 ,80 The increase in working time when a student was present, as reported by FPs, ranged from 30 to 120 min.62 ,82 ,85 The observed and timed difference in consultation activities of teaching FPs with their non-teaching colleagues was 1.23 h.83 No differences were reported regarding number of patients, charging/billing of patients, performing of practical procedures and ordering of diagnostic tests between FPs’ visits with and without a student.79 ,80 One study that had a low response rate, reported no decrease in clinical productivity (number of patients/hour) or overtime hours, while clinical productivity correlated to the number of patients seen independently by the student.28
Impact on patients in the teaching practice
The impact on patients was reported by eight papers from the UK,86–88 the USA,31 Australia,89 Israel,90 Sweden91 and Austria29 (table 6). All of them used questionnaire surveys with attitudinal statements and Likert scales and are non-comparative, except for two studies where patients seen with students were compared to those seen without students or before and after the consultation with a student.88 ,89 Questionnaires were locally developed and piloted, but no validation was reported. Only one study adapted an already validated questionnaire.88
The majority of patients do not report a negative impact on the quality of their FM consultation when a student is involved29 ,31 ,86 ,90 ,91 and would not refuse a student.86 ,89 ,90 ,91 Validated scores for enablement and empathy were not significantly different between patients who had a consultation with a student present and those without.88 Patients in some studies even reported some advantages when a student was present such as getting a second opinion, better explanations, more time to talk about the problem and a more thorough history taking and examination, as well as personal satisfaction and self-esteem due to contributing to education of future physicians.31 ,86 ,88 ,90 ,91 In an Australian study, patients would accept more involvement of the student in history-taking, physical examination or procedures than expected by them before or occurring during the consultation.89 In Sweden, some of them felt they could contribute to teaching through being facilitators of the development of students’ skills and attitudes, exemplars and experts of the medical condition, as well as providing a real context for learning.91
In some studies, a small number of patients (1–6%) reported a negative effect of the student’s presence during the consultation, such as longer consultations31 ,86 ,91 or more difficulty/less space to talk about personal problems.87 ,91 Although one study reported a significant difference in length of consultations with and without students present as recorded by the FPs,88 in other studies, the majority of patients did not think that either their consultation took longer when a student was present29 or that time with their FP or the FP’s attention was reduced due to the presence of a student.31 ,87
Discussion
Summary of main findings and comparison with previous reviews
This systematic review on the impact of FM clerkships in undergraduate medical education found that they are highly valued by students and overall well-accepted and even beneficial to the teaching FPs and their patients. The 64 reviewed studies reported from a wide range of countries with both well and less-developed academic and clinical FM. None of the reviewed studies evaluated an impact beyond the Kirkpatrick outcome level 3 and only one study achieved grade 5 of the BEME’s strength of findings.
The reviewed studies reported students’ satisfaction with both the content and process of teaching and learning in FM clerkships. The main contributions are the variety of common clinical experiences encountered including chronic, continuity and preventive visits; integration of previous learning and further development of communication and focused physical examination skills; becoming familiar with the organisational and business aspects of the medical practice as well as developing a biopsychosocial approach to patient care, looking at the patient not as a disease but as a whole person in the context of the family and community. Students value the enthusiasm and positive attitude of teaching FPs and their staff that leads to quality teaching. Based on the few studies that assessed knowledge and skills, the FM clerkship enhanced previous learning in other specialty clerkships and provided unique learning, especially on dealing with common acute and chronic conditions, health maintenance and disease prevention, communication and problem-solving skills.
The teaching and learning experiences in FM clerkships seem to improve students’ attitudes towards this specialty, and influence their career intentions and decisions. Yet this new or enhanced interest in a FM career due to the clerkship does not persist without change. While the FM clerkship experience is important to counteract students’ negative stereotypes about FPs and their work, and inform career choice, a definitive career shift to FM requires a comprehensive and complex intervention package due to the broad scope of factors that influence the specialty choice process from premedical school into practice life.40 ,92 ,93
Although there is variability in clerkship settings and countries, the overall message is that FM clerkships provide a valuable and satisfactory educational experience for medical students with the main contribution not in a unique list of diagnoses or procedures, but in a different approach to practicing, teaching and learning medicine derived from the person-centred system-based worldview of FM.60
Teaching FPs report increased job satisfaction and stimulation for professional development due to involvement with students. They also recognise some negative impact in their work as a result of teaching such as increased workload and less productivity, although findings are not consistent. Patients in FM practices involved in FM clerkships are open and willing for students to observe and participate in their consultations. Overall, student’s presence and participation has a positive impact and increases patients’ satisfaction with their consultations, and there is room for even more active involvement of both patients and students.
Previous reviews on teaching and learning in ambulatory care in North America have reported its positive contribution in the education of medical students, while emphasising the variety of settings, measurements and outcomes used by different studies, and the low number of studies applying rigorous methods to evaluate educational outcomes.16–18 Our systematic review was the first, to our knowledge, focusing specifically on the impact of FM clerkships, and it covered a longer timeline (1990–2013) and included a wider spread of countries. We noticed an increase in studies on the impact of the FM clerkships in countries where this discipline does not yet have a clearly defined status in the healthcare system or is under development. This reflects the pursuits to strengthen FM and primary care in these countries and the need for further data to support its integration in the basic education of future physicians.
The rigour of research on the evaluation of ambulatory care educational outcomes has been previously reported as weak, especially in regard to limited tools used to measure learning outcomes and the lack of generalisability.17 ,18 Our review assessed the quality of studies’ findings with the BEME grades of strength and the Kirkpatrick outcome evaluation levels that were not used in previous reviews of ambulatory care teaching and learning. Our findings show that quality of research on evaluation of FM clerkships is still weak, even though medical education research and practice on assessment and evaluation tools has been growing rapidly in the past decade.94
Most of the studies that evaluated the impact on students used self-assessment through locally developed instruments (patient encounter logs, evaluation or attitudinal questionnaires), without reports of validity and reliability. Very limited adjustments were made for the patient mix of different FM practices, locations and seasons, as well as the timing of the clerkship on the academic year and prior learning in other clerkships. This limits the generalisability of findings to other institutional, educational and patient care settings. Studies that evaluated the impact on teaching FPs and/or their patients used mainly self-designed instruments without a thorough validation and with limited adjustment for physician-to-physician variability in clinical and teaching experiences and patients’ mix. Most of the studies relied on self-reporting by FPs and patients, and only a few attempted direct observation or validation from other sources.
None of the reviewed studies reported changes in organisational practice or improvement in patients’ health outcomes as a direct impact of learning in FM clerkships, yet this is common in medical education reviews.24 This is to be expected, as such a level of evaluation requires a long follow-up and it is impossible to adjust for the complexity of factors that influence the practice of patient care besides the basic education of the practicing FPs.95
Even in the light of these methodological problems and differences in organisation and evaluation of FM clerkships in the reviewed studies, the overall consistency of results across different studies and countries supports the generalisability of findings about the positive educational impact of FM clerkships.
Strength and limitations
This systematic review was based on a comprehensive search strategy using the PRISMA guidelines and included the major databases for medical and educational research. The reviewers had previous experience with medical education research and come from well and also from less-developed settings of clinical and academic FM. The lack of meta-analysis is a limitation of this systematic review, but this was not possible due to the variety of study designs, tools and outcomes used, and the nature of reported results. As all reviewers are FPs, passionate for clinical and academic FM, this may have introduced bias in the analysis and synthesis of results. Owing to language and accessibility limitations, the review may have missed other studies published in this research area.
Implications for future practice and research
Research on the impact of FM clerkships in countries with a less-developed status of this discipline has been gradually growing in the past decade. Yet, it should not just repeat, but rather build on the lessons learned by research in countries with a developed status of FM, the best current recommendations on assessment and programme evaluation, as well as the local context and culture. Future studies that include different medical schools and countries, and use standardised and validated evaluation tools would increase the generalisability of the current findings and determine best interventions and practices in FM clerkships.
Triangulation and comprehensive evaluation involving the different stakeholders of FM clerkships such as students, teaching FPs and patients, medical school and healthcare institutional leadership, other primary care or hospital-based specialists, other staff in teaching FM practices, etc, need to be the focus of future studies. This becomes very important in light of the ‘chilly academic climate for primary care’ and the ‘cultural bias against primary care’ in some medical schools and regions.96–98 The negative attitudes of hospital specialists toward the involvement of FPs in undergraduate medical education may not only be due to ‘specialty rivalry’ for curricular time, teaching resources and academic prominence, but also due to the differences between the ‘health and care’ approach of primary care and the ‘disease and cure’ approach of secondary/hospital care.60 ,96 ,99 The resistance towards FM and its development with the increasing involvement and contribution of FM in undergraduate education needs to be further explored in future studies. This would provide a more comprehensive view of the impact of FM clerkships and further insight for countries where FM is still in the early stages of pursuing entrance and acceptance into the medical academia.
In light of previous reviews suggesting longitudinal versus block ambulatory clerkships to ensure more continuity of patient care and student-teacher relationship,17 and recent reports on the value of longitudinal integrated clerkships,19 ,100 future research should also focus on longitudinal FM clerkships and their contribution in the education of future physicians.
Acknowledgments
The authors would like to thank Mrs Cil Leytens at the Department of General Practice, University of Antwerp, for her valuable help in retrieving some of the full-text papers and Dr Elizabeth Swain in Scotland, UK, for the English language editing. The authors would also like to acknowledge the JOIN-EU-SEE Erasmus project of the European Union as the idea and the work for this paper developed during a visit of ET at Department of General Practice, University of Antwerp, in November 2013, which was funded by a JOIN-EU-SEE staff exchange scholarship.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors ET and RR developed the idea for the study. ET, RR and NRM developed the search strategy and ET performed it. ET, RR, NRM and KH were all involved in the review of the papers. ET drafted the manuscript. RR, NRM and KH commented on the manuscript. All the authors read and approved the final manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.